CHONDRITIS AURICULA
I Made Nudi Arthana
Chondritis auricula often time due to by infection bacteria Which attacks the ear cartilage. Other risk factors include open wounds to the ear, medical procedures such as ear piercing, or autoimmune diseases. Inflammation is the main cause of chondritis, which can be caused by trauma to the leaf ear (auricle) consequence wound burn, surgery, piercing ear, or blunt or sharp trauma such as in wrestling matches or acupuncture. One of the complications of perichondritis that spreads deeper into the chondrium to become chondritis. . 1- 14
LITERATURE REVIEW
Anatomy And Physiology Outer Ear
The outer ear consists of the auricle and the external acoustic canal. 8 The auricle is a symmetrical right and left cartilage frame that functions to focus or localize sound. The auricle consists of the conchae, the tragus in front, the antihelix above and behind and the antitragus below. The helix extends superior and posterior from the crucible helical up to lobule surround antihelic, concha and antitragus. Between the helix and antihelix is the scaphoid fossa. Triangular fossa is at between crucible superior And crucible inferior from the antihelix. Leaf The ear is anchored to the cranium by skin, cartilage, ear muscles and extrinsic ligaments. 8,9
The external acoustic canal consists of a lateral third and a medial two-thirds. The external acoustic canal is 2.5 cm long with a volume capacity of 1-2 ml. The lateral third of the ear canal is formed of fibrocartilage. And two third medial is bone. During time toddler form The external acoustic canal is straight but then becomes “S” shaped at the age of 9 years. 8,9
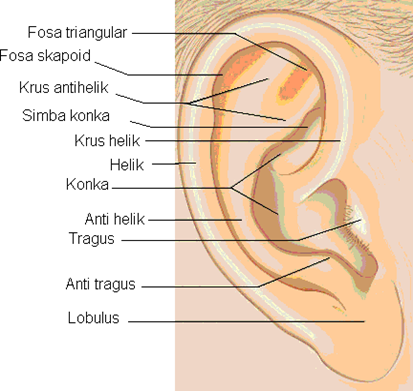
Picture 1. Anatomy earlobe . 8
The external acoustic canal has an important relationship with the mastoid segment. from nerve facialist, Which is at in behind from canal This when walk down towards the stylomastoid foramen. The temporomandibular joint is located in front of the external acoustic canal so that disease processes affecting the temporomandibular joint can cause referred ear pain. 8
The external acoustic canal is lined by stratified squamous epithelium that is continuous with the skin of the auricle and the epithelium covering the tympanic membrane. The subcutaneous layer of the cartilaginous part of the ear canal contains hair follicles, sebaceous and cerumenous glands and is up to 1 mm thick. The skin of the osseous part of the ear canal has no subcutaneous elements and is only 0.2 mm thick. The epithelium of the external acoustic canal has the ability to migrate laterally to keep the ear canal free from debris. The migration rate of the epithelium is 0.07 mm/day and is thought to occur in the basal cell layer. Cerumen glands are modified apocrine sweat glands that are surrounded by myoepithelial cells and arranged as apopilosebaceous units. Cerumen provides a hydrophobic layer for the canal. ear. Earwax can functioning as antibacterial And normally own The pH is acidic and is an environment that germs do not like. 8

Picture 2. Cross section cartilage leaf ear. 1
Leaf ear And canal acoustician external innervated by branch auriculotemporal from the mandibular division of the trigeminal nerve, the greater auricular nerve from the cervical plexus, the auricular branch of the vagus nerve, namely Arnold's nerve, and branches of the facialist And glossopharyngeus. Part lateral, medial And posterior ear innervated by the greater auricular nerve. Arnold's nerve innervates the osseous part of the inferior ear canal, the cartilaginous part of the posterior superior ear canal and the corresponding segments of the tympanic membrane and conchae. The inferior ear canal posterior superior is innervated by branches of the facial nerve. 8
The anterior and superior walls of the ear canal and tragus drain into the preauricular lymph nodes. The infraauricular lymph nodes drain from the helix and inferior wall of the ear canal, while the conchae and antihelix drain into the mastoid lymph nodes. 8
The posterior auricular artery and the auriculotemporal branch of the superficial temporal artery arise from the external carotid artery and supply blood to the auricle and lateral ear canal. The deep auricular branch of the maxillary artery supplies blood to the Which more medial from hole ear And surface outside from membrane tympani. The posterior auricular and superficial temporal veins drain the ear canal. The posterior auricular vein is continuous with the sigmoid sinus. 8Ear outside help transmission voice Which effective to membrane timpani
by acting as a functional resonator. The acoustic contribution of the outer ear is to enhance the transmission of sound at speech frequencies. The depth and curvature hole ear protect membrane timpani, structure ear middle And inner ear. Hair in canal acoustician external part outside prevent entry small foreign objects and foreign debris. 8
Definition
Perichondritis is inflammation of the cartilage and ear that occurs when trauma or inflammation causes an effusion of serum or pus between the layers of the perichondrium and the ear. cartilage ear outside. Generally trauma in the form of laceration or consequence damage which is not incidental to ear surgery. Occasionally perichondritis occurs after a bruise without hematoma. In the early stages of infection, the pinna may become red and tender. This is followed by generalized swelling and formation of a subperichondrial abscess with pus collecting between the perichondrium and the underlying cartilage. 1 ,2,3
Chondritis is an inflammation of the cartilage. Chondritis can occur in any area Which own cartilage like ear, nose, larynx, trachea, And Also joint area. Cartilage in pinna auricle formed by elastic cartilage. 10 Auricular chondritis is an inflammation of the auricle cartilage that causes an effusion of serum or pus between the perichondrium and the ear cartilage. 11
Othematoma, also known as auricular hematoma, is a collection of blood blood in lower layer perichondrium ear Which generally caused by trauma. 12 This condition can occur as a result of various types of trauma, including ear piercing, although it is more common as a result of greater force or a direct blow to the ear, such as in a motor vehicle accident. Hematoma auricularis Also can happen as consequence from activity sport contact, such as wrestling, boxing, and martial arts. 13
Etiology
The most common pathogen causing perichondritis is Pseudomonas aeruginosa, followed by Staphylococcus aureus, Proteus mirabilis and other gram-negative organisms. 1,3
Factor predisposition :
Inadequate on therapy cellulitis leaf ear (pinna) And otitis external I.
Accidental or surgical (after aspiration or incision hematoma leaf ear).
Infection secondary from laceration or hematoma
Infection superficial acoustic meatus .
Wound burn or frostbite.
Stabbing earrings on bone vulnerable, can cause happen Streptococcus beta hemolytic septicemia. 2
Inflammation is the main cause of chondritis, which can be caused by trauma to the earlobe (auricle) due to burns, surgery, ear piercing, or blunt or sharp trauma such as in wrestling matches or acupuncture. Complications of perichondritis that spread deeper into the chondrium. 14 Auricular chondritis is a disease caused by infection. Bacteria that most general cause perichondritis And chondritis auricularis is similar to Pseudomonas aeruginosa and Staphylococcus aureus. Escherichia coli can also cause chondritis.
The most common etiology of auricular hematoma is blunt trauma to the ear. This condition can occur as a result of contact sports accidents, such as wrestling, boxing, martial arts, football, or rugby. In addition, earring insertion and motor vehicle accidents can also cause auricular hematoma. 15 Although rare, several case reports have reported the occurrence of auricular hematoma that was not caused by trauma, or non-traumatic. A study reported hematoma auricle spontaneous with beginning I. Besides That, There is also a study reporting two cases of auricular hematoma due to mobile phone use.16
Pathophysiology
Perichondritis
Trauma to the auricle is the most common predisposing factor for perichondritis of the auricle. Trauma to the auricle can be trauma sharp which causes wounds, and blunt trauma. Then it happened inflammatory reaction with 5 cardinal signs in the form of pain or painful, rubor or reddish, heat or hot, tumor or lump and dysfunction or disruption of the function of the organ that is inflamed. 1,9,17 Pathogens reason perichondritis sequentially from Which most frequent that is: Pseudomonas aeruginosa, Staphylococcus aureus, Enterobacter, Proteus mirabilis, and other gram-negative bacteria. Approximately 90-95% of the causative organisms is Pseudomonas. This pathogen infects after existence predisposition previously for example trauma leaf ear and spread of infection around the earlobe. 17
Process the occurrence inflammation on every wound on network will arise inflammatory reaction, where the blood vessels will dilate so that moment inspection will looks red and feels warm on palpation. Initially there is local dilation of the arterioles and capillaries so that plasma will seep out. Furthermore, edema fluid will collect in the area around the wound, so that a lump will form, the collected fluid will press on the nerves, so when palpated there is usually also flavor painful, Then fibrin will form kind of net, structure This will cover the lymph channels so that the spread of microorganisms can be limited. 17
This inflammatory process also occurs in blunt trauma, However, in relatively blunt trauma that does not cause wounds, there is no process of removing fibrin threads. Superficial infection from the external ear canal or from the auricle spreads deeper into the perichondrium. In this condition, it is called the early stage, the auricle ear (pinna) red And painful Then start formed abscess subperichondrial. This causes the cartilage to lack blood supply, resulting in necrosis. cartilage so that deformity can occur in the earlobe which is called cauliflower. 18,19
Chondritis
Trauma to the auricle can develop into a more severe infection that threatens the survival of the underlying cartilage due to the lack of direct vascularization. After initial trauma to the auricle, blood or serum collects in the subperichondrial potential space and secondary infection by S. aureus, P. aeruginosa, and Proteus species can occur. Chondritis can also occur as a complication of ear surgery or otoplasty. Undetected or inadequately drained hematomas in the postoperative period can cause chondritis. Perichondrium is barrier Which very Good For prevent distribution infection, but If happen distribution more in, so can happen chondritis. 26
Othematoma
The auricle consists of skin, subcutaneous tissue, muscle, and perichondrium that supplies blood to the underlying cartilage, an auricular hematoma is a collection of blood between the perichondrium and the underlying cartilage. The main areas of cartilage in the ear covering tragus, helix, antihelix, fossa triangular, conch cymbals, And concha cavum. The blood vessels supplying the ear consist of the superficial and posterior temporal auricular arteries. In ear trauma, the perichondrium and blood vessels are damaged, causing separation from the underlying cartilage and creating a potential space for blood to accumulate. Once blood fills this space, it causes vascular compromise of the adjacent cartilage and congestion vein Which can cause change histological And abnormality subsequent cartilage formation, resulting in an unsightly appearance of the outer ear known as cauliflower ear, there is a process of neocartilage development which is a change in the normal histological structure of the ear cartilage framework. 22,24
In general normal injury network or existence material foreign become trigger events involving enzymes, mediators, extravasated fluid, cell migration, tissue damage and healing mechanisms. This condition can cause signs of inflammation such as redness, swelling, heat, pain and loss of function. Occurs 3 process main during reaction inflammation This that is, flow blood regional This increases, capillary permeability increases, initially white blood cell components such as neutrophils and macrophages, then followed by lymphocytes exiting the capillaries. lead to network. Next move to the injury site under the influence of stimulus – stimulus chemotactic. When There is antigen the, at first response immune non-specific mechanisms work to eliminate the antigen. If this mechanism is successful, inflammation I stop. If response immune non specific No succeed, so Specific immune responses are activated to ward off the antigen. However, if these mechanisms fail, the inflammation becomes chronic and often causes irreversible destruction of the tissue. 23,25
Symptom And Sign Clinical
Perichondritis
On area auricle Which caught trauma at first arise flavor Sick or hot which is getting longer getting better then there is a reddish swelling followed by a feeling pain. Swelling can occur immediately or several hours after trauma so that the contour of the auricle disappears. The onset of perichondritis is characterized by redness swelling Which evenly on leaf ear and causes pain. The earlobe feels hot And painful If touched. Edema can spread to area behind ears and causes earlobes protrude (tense/tender). The formation of abscess, usually Also found fever, enlargement gland lymph regional, And leukocytosis. Serum pooling in the subperichondrial layer occurs immediately purulent, causing local fluctuation or diffuse. Skin on area the infected will form crust with squama debris And start blister when it comes to cartilage. Ear experience induration, erythema And often time hole closed ears by due to edema. Contour auricle disappear And edema generally found in area conchae. Areas that do not have cartilage such as lobules still persist. Edema extends to area behind ear cause auricle pushed even edema Can extends to the face. 20,27


Othematoma
Auricular hematoma or othematoma is commonly found in patients with a history of trauma to the auricle. Patients with othematoma have clinical symptoms of edema or swelling. on leaf ear consequence from blood Which clot in between perichondrium and network soft in part front ear. There is painful on ear, feel heat in the ear. Other complaints such as fever may be found as a sign of infection, painful after trauma as well as bleeding, necrosis on part Which caught trauma caused by loss of adequate nutrition and this condition will trigger irregular fibrosis and cartilage formation around various cartilage components. Symptoms can be severe to hearing loss, tinnitus or ringing in the ears, headache, blurred vision, swollen face. 28
As a result, structure ear Which usually sunken will become full with connective tissue. The cartilage then changes shape and curves and causes a type called Cauliflower Ear. Rapid evacuation of the hematoma can restore the closure of the cartilage and perichondrium, thereby reducing the possibility of deformation. 26Hematoma usually fills the space between the helix and antihelix (scapha) and extends to front to in fossa triangular. Hematoma can occupy conch or the area in and around the external auditory meatus. It is important to note that hematomas auricular Also can happen on surface posterior ear or may involve both anterior and posterior surfaces. The risk of necrosis is greater if the hematoma is on both the anterior and posterior surfaces. The overlying skin may be normal in color or may be erythematous or ecchymotic. The skin is usually intact and the hematoma is soft to palpation. 26

Picture 4 . Appearance Clinical Auricular Hematoma Dextra 28
Chondritis
Piercing ear in outside by power No professional often done And become one of reason most frequent from perichondritis as well as chondritis. Symptom clinical Which can what happened is painful on part Which infected, reddish, swollen, there is pussy or fluid, fever as sign infection, as well as deformation from structure on case Which heavy. Systemic symptoms that may occur are pyrexia or erythema that extends to the pinna as a sign of infection that has spread to the external ear. 29

Picture 5 . Description Clinical Chondritis I Left Auricular 23
Diagnosis
Perichondritis
Diagnosis perichondritis can enforced based on anamnesis And inspection physical. Anamnesis
In the anamnesis, there was a history of direct blunt trauma to the auricle. A history of auricular trauma is important for establishing a diagnosis of perichondritis because it originates from injury to the auricular cartilage. Complaints are generally pain in the auricle. after trauma. Leaf ear swell, colored reddish, feel heat, pain, sometimes accompanied by fever, and enlargement of regional lymph nodes.
Inspection physique
It is characterized by edema, fluctuation, tenderness and the contour of the auricle begins to disappear. Edema Which wide on auricle, hyperemia, feel hot, painful press, there is fluctuations when suppuration occurs, there is deformity If necrosis has occurred, regional lymph nodes will enlarge.
Inspection support
In supporting examinations, laboratory examinations can be carried out. Routine blood tests can show leukocytosis. In culture examinations for determine bacteria reason infection. Test sensitivity For determination antibiotics that appropriate in accordance bacteria reason. On otoscopy membrane timpani looks normal. Audiometry examination showed no hearing loss. 18,19,20
Othematoma
The diagnosis of auricular hematoma can be made clinically. Patients generally have history trauma blunt on ear. Important asked things specific which can trigger othematoma such as trauma, ear pain, previous events, whether there is fever/chills, drainage from the ear, whether there are changes in hearing, immunosuppression, diabetes, blood thinners, and hypertension. If mechanism trauma considered heavy, like on accident motor vehicle or head trauma, then there is temporal bone trauma and emergency need removed moreover Formerly. Inspection support No routinely performed in cases of auricular hematoma. 22
Patient with auricular hematoma generally come to facility health with symptoms swelling on ear part anterior, Which accompanied by painful pulsating mild to moderate. In addition, patients often have a history of previous ear trauma. 12 Systematic symptoms such as fever, chills, and hearing loss hearing Also need evaluated on patient hematoma auricle. Complaint history repetitive, immunosuppression, diabetes, use thinner blood, And Hypertension also needs to be evaluated in patients. 23,28
Physical examination of the external ear is usually sufficient to diagnose an auricular hematoma. However, a complete head and neck examination is necessary to evaluate for other organ damage, especially if the auricular hematoma involves a head injury. 2,13 Basic knowledge of ear anatomy is necessary to evaluate the external ear. Otoscopic examination is necessary to evaluate the condition of the external ear canal and tympanic membrane. Hematomas are generally found between helix and antihelix, can spread on antihelical fossa. However, in some cases, hematoma can fill the concha, external auditory meatus, or posterior part of the ear. 12
If the hematoma occurs in the anterior and posterior ear, there is a risk of necrosis generally more big. Skin generally intact And hematoma will feel soft to palpation. After 24 hours, the blood will clot and the hematoma will be more pronounced. hard. On hematoma auricle Which No handled, cartilage on ear will disappear And experience fibrosis. Matter This Then cause description cauliflower ear. 28 In cases of trauma to the ear, an evaluation of the condition of the head is also required And neck. Trauma bone temporal need evaluated For possibility fracture. Evaluation of the facial nerve is also necessary for possible damage due to its proximity to the ear. 12
Inspection support seldom required on hematoma auricle. Supporting examinations can be used to rule out differential diagnoses and look for complications. 12 Ultrasound examination can be used to rule out differential diagnoses of auricular abscess and evaluate swollen ears. Examination CT scan or MRI Possible required on condition trauma ear suspected foreign body involvement, evaluation for possible abscess, evaluation of the middle ear And in, as well as evaluation intracranial If hematoma auricle involving injury head. 4.13
Chondritis
Chondritis can diagnosed with anamnesis Which focused, as well as inspection thorough physical examination. History should include whether there is trauma to the lateral face and ear. There is a history of trauma to the auricle, a history of surgery to the auricle, both of which are the result of cartilage injury. The patient complains of symptoms of chondritis such as pain and heat in the auricle . 5
On physical examination, swelling of the ear, erythema, discharge of serous fluid or purulent exudate from the affected cartilage, and increased corner auriculocephalic. 24 For help enforcement diagnosis auricular chondritis can be cultured and tested for sensitivity to determine the causative microorganism. Chondritis and perichondritis can also be distinguished by biopsy. In patients with chondritis, the biopsy results can find necrotic cartilage. 13
One way to establish a diagnosis of chondritis is with ultrasonography, as well as CT-Scan. Ultrasonography findings in patients with auricular chondritis before starting treatment showed soft tissue swelling in around cartilage And network soft perichondral with improvement Power Doppler Signal (PDS) that is consistent with the biopsy findings. In addition, FDG-PET/CT also shows an increase in Fluorodeoxyglucose (FDG). 25
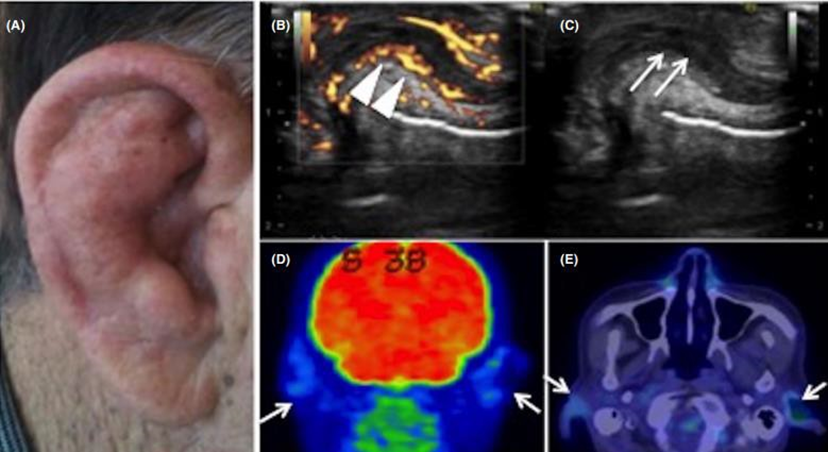
Picture 6 . Ultrasonography And CT Scan Patient with Chondritis Auricularis. 25
Inspection blood routine usually No done, However If There is area swelling that expanding, abscess or necrosis so need done test blood including count complete blood count, urea, electrolytes, C-reactive protein, blood culture and coagulation screening. Imaging is not indicated unless there is suspicion of intracranial pathology such as an abscess.
Management
Perichondritis
Management of auricular perichondritis includes antibiotic therapy, drainage and debridement. on time Which appropriate For save cartilage Which Still life. In early cases perichondritis can be treated with oral fluoroquinolones. 19,31,32
The earlobe and ear canal should be cleaned carefully and thoroughly. Ointments containing antibiotics and antiseptics can be applied topically and the taste is painful controlled with drug anti-inflammatory non steroids. When response to non-surgical therapy is not successful within 48 hours or if the disease has progressed, which is indicated by the presence of an abscess, then surgical treatment is carried out in the form of an incision and drainage auricle. 19.30 Objective Handling surgery the is For reduce necrosis cartilage And minimize deformity in Then day 18 A number of method for avoid deformity Which often happen after a method incision simple repetitive, that is method excision Which introduced by Stroud And method through pipe drainage and through Which introduced by Stevenson. Bassiouny introduced a new method that is a combination of the two methods above. The Stroud technique involves excision of the diseased cartilage along with the anterior skin and the overlying perichondrium. Dowling et al., have used this method to treat early stage perichondritis localized in the antihelix and reported minimal deformity when the helix is intact. 33
Stevenson introduced a method for treating cases of perichondritis after end aural incision . Two inserted perforated rose pen pipe , one anteriorly and one posteriorly with the ends of the tubes stitched through each tube. The tubes are injected with an anti-pseudomonas antibiotic fluid such as bacitracin.
50.00 U dissolved in 250 ml of physiological solution or gentamicin drops twice a day. 20,33
Intravenous systemic antibiotics can be given for 1-4 weeks. If production abscess has stop, pipe lifted slowly every 2 day. But one of the vertical pipes can be maintained for up to 4 weeks. 18.33
Penetration into cartilage is good and high activity against Pseudomonas aeruginosa makes ciprofloxacin the drug of choice besides being able to fight Staphylococcus sp . Ciprofloxacin is the antibiotic of choice for perichondritis combined with anti-pseudomonas drops such as gentamicin or fluoroquinolone drops. Intravenous administration using pseudomonas-sensitive antibiotics can be started when the infection has spread to involve the surrounding soft tissue and lymph flow. For the treatment of advanced cases involving surrounding tissue and the presence of lymphadenopathy, intravenous ceftazidime or fluoroquinolone is needed. 5 The choice of antibiotics should be adjusted to the culture results. Antibiotics can to be continued For a number of day after seen healing Which real due to the possibility of hidden residual infections. 6
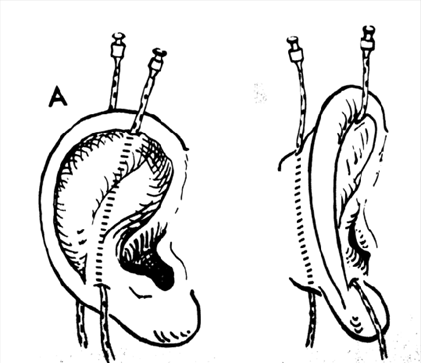
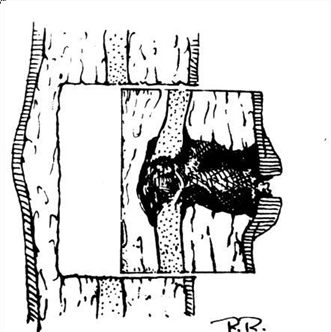
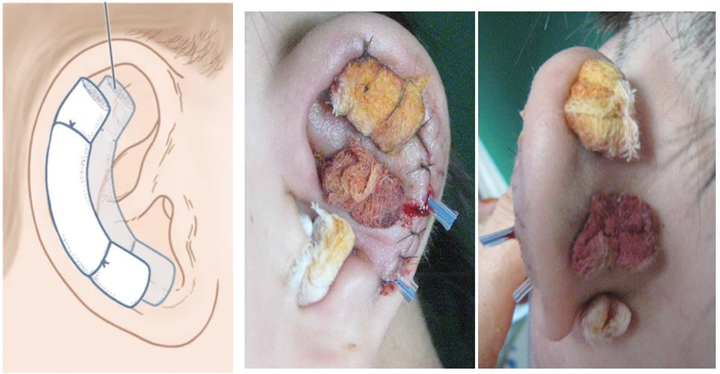
Picture 7. (a) Method Stevenson (b) Method Stroud 33
The advantage of the drainage method is that the tube also acts as a scaffold that prevents the occurrence of perichondrium wrinkles so that the new cartilage that is formed will be homogeneous and prevent the cauliflower from expanding further. assisting antibiotic irrigation measures to in the subperichondrial space against sensitive organisms and will not be potentially toxic because it is not administered systemically. Thus this method of tube drainage should is method choice for all case perichondritis And method excision is increasingly being abandoned. 33
Othematoma
After hematoma diagnosed, important For to discuss with patient regarding risk, benefit, And alternative treatment. If hematoma happen in condition I
< 48 O'clock, effort drainage is appropriate. Need remember that patient can choose to withhold acceptable treatment as long as the patient is aware of the risks and possible poor cosmetic results if treatment is not performed. 35
Step Procedure General For Drainage Hematoma Auricular:
A local anesthetic should then be injected or applied topically to the site where the incision or aspiration will be performed (e.g., lidocaine, bupivacaine, LET gel). For results best, anesthesia can injected in pattern block auricular or directly to the auricular hematoma site. A few minutes after injection, the level of anesthesia local must assessed. There is two method Which can used For
remove auricular hematoma. One method is to perform an incision and drainage of the hematoma using a scalpel, while the other method is needle aspiration. 12d
Incision and drainage:
Make a linear incision that can be made in the skin over the swelling or hematoma. The purpose of the incision is to drain the fluid collection; however, making the incision in a cosmetically pleasing location is ideal. The incision at area sunken will healed with results Which more aesthetic compared to with convex area.
After incision made, hemostat And suction can used For evacuate the hematoma.
Once all the hematoma has been removed, the area can be flushed with normal saline solution.
Wrapping tampon installed. Tampon functioning For close room dead or potential space where hematoma can form. When using dental rolls as tampons, two rolls should be used. Each roll should be positioned so that it is parallel to the incision line on either side of the ear. Two vertical sutures should be placed to secure the tampon. However, it is important to make the sutures loose enough to maintain the blood supply of the ear.
Bacitracin can smeared on location incision after procedure. 12

Aspiration :
Procedure alternative use needle size 18 For to aspire hematoma. Several studies have shown that an 18-gauge needle is acceptable for evacuation of auricular hematoma when the hematoma is less than 2 cm. If using the needle aspiration technique, a tampon should be placed over the affected ear area after complete removal of the hematoma.
A tampon is placed. The tampon serves to cover the dead space or potential space where the hematoma can form. When using dental rolls as a tampon, two rolls should be used. Each roll should be placed so that it is parallel to the incision line on either side of the ear. Two vertical sutures should be placed to secure the tampon. Adequate tamponing is applied when there is no potential space for hematoma to accumulate; however, important For make stitches Enough loose For guard supply ear blood vessels.
Bacitracin can smeared on location incision after procedure. 12

Picture 9 . Technique Aspiration Needle For evacuation hematoma 2 Tampons Post Hematoma Evacuation:
There are some differences in the types of tampons used, but the goal remains the same, which is to eliminate the space that allows fluid to build up. New approaches include the use of tampon materials that can be molded to the shape of the vagina. ear shape. A recent cases this is reporting use glue fibrin to attach the perichondrium to the cartilage, thereby reducing the risk of separation. This tampon can be removed after 5 to 7 days. The use of antibiotics is left to the discretion of the physician. If cauliflower ear does form, excision with repair can be performed in the form of otoplasty. 36
Picture 10 . Use Tampon post evacuation hematoma. 36
Chondritis
The goal of management of chondritis is to eradicate infection and optimize outcomes. end cosmetics from ear patient. Management treatment consists of from administration of antibiotics, repeated surgical debridement, and local wound care. Administration of antibiotics given For bacteria grams negative And S. aureus. Antibiotics This can consists of antipseudomonal aminopenicillin or fluoroquinolone for 2-4 weeks. 14
In the mild stage, debridement and treatment with oral and topical antibiotics are sufficient. If this therapy is unsuccessful, debridement and culture are performed. Provide appropriate treatment according to the culture results. Ciprofloxacin is a suitable choice for the moderate stage, combined with anti-Pseudomonas eye drops such as gentamicin or ciprofloxacin. 11 If the infection has spread to the soft tissue and regional lymphatic system, the patient must be hospitalized And can given treatment parenteral For overcome infection Pseudomonas. Intravenous ciproplocacin or ceftazidime can be given. Crusts on the auricle can be cleaned with hydrogen peroxide. 14 The goal of surgery is to eliminate necrotic cartilage tissue and minimize deformity that may occur. The affected area is cleaned and given local anesthesia and epinephrine. If the entire auricle is involved, a total pinnectomy is justified. Surgical techniques vary from complete cartilage excision to bivalve incisions along the sides of the auricle to insert multiple tubes for antibiotic irrigation. However, only isolated cases are suitable for this technique. The tubes can be used for 1 month with antibiotic irrigation. 24
Prognosis
The sooner it is diagnosed, the better the aesthetics, which are limited to non-deforming hypotrophic scars. However, if cartilage necrosis has occurred, the aesthetics are not good. Aesthetic reconstruction can be done, but it must be waited for to be sure that the remaining infection has completely disappeared. 1,11
The prognosis for auricular hematoma is generally good if immediate action is taken. Complications hematoma auricle is formation network cartilage new And fibrosis that cause deformity, the main thing cauliflower ear. 12 If diagnosis enforced early and start giving antibiotics, it is expected to be completely cured. In advanced cases, some parts of the ear may experience necrosis and surgery must be performed. So that in the end, reconstructive plastic is needed to restore the normal shape of the ear. 11
REFERENCE
Ha Richard Y, Trovato M.J. Cauliflower Ears. In: Plastic Surgery of The Ear. Dallas, 2011; p.1-46.
Khan Najeed, Cunning Nina. Pinna Perichondritis. National Library of Medicine. 2023.34283447
Chang C. Cauliflower Ear and Auricular Hematoma. Fauquier Ear Nose and Throat Consultants of Virginia. Downloaded from: URL:http://www.fauquierent.net/cauliflowerear.htm .
Timothy Kindergarten, Tae Hoon Jinn. Diseases of The External Ears. In: Ballenger,
J. J, editor. Otorhinolaryngology Head and Neck Surgery. 16th ed. London. Hamilton, 2013; p.230-47.
Lalwani AK.Disease of the External Ears. In: Current Diagnosis & Treatment in Otolaryngology Head and Neck Surgery. 2nd Edition. Mc Graw Hill, 2007;p.345-67.
Greywood JD, Pribitkin EA, Crein H. Management of Auricular Hematoma and the Cauliflower Ear. Facial Plast Surg. 2010;26(6):451-5.
El-Bestar MF. Surgical Treatment of Cauliflower Ear. J. Plast Reconstr Surg. 2004;28(1):23-7.
Lalwani AK. Anatomy and Physiology of the Ear. In: Current Diagnosis & Treatment in Otolaryngology Head and Neck Surgery. Edition 2nd. Mc Graw Hill, 2007; p.305-22.
Moller AR. Anatomy of the Ear. In: Hearing - Anatomy, Physiology and Disorders of the Auditory System. 2nd Edition. Texas, 2006; p.11-7.
Chan Y, Goddard JC. KJ Lee's Essential Otolaryngology [Internet]. 11th ed. 2015 [cited 2023 Jul 3]. Available from: https:// www.worldcat.org/title/904528570
Khan N, Cunning N. Pinna Perichondritis. StatPearls [Internet]. 2023 Jan 2 [cited 2023 Jul 3]; Available from: https://www.ncbi.nlm.nih.gov/books/NBK572081/
Krogmann RJ, Jamal Z, King KC. Auricular Hematoma. New England Journal of Medicine [Internet]. 2022 Aug 1 [cited 2023 Jul 3];383(19):1867–77. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531499/
Auricular Hematoma - Emergency Management [Internet]. DynaMed. 2023 [cited 2023 Jul 3]. Available from: https://www.dynamed.com/management/auricular-hematoma-emergency- management#GUID-62FE712A-1AD8-4563-A006-2DD874A6F012
Snow JB, James B, Wackym PA, Ballenger JJ. Ballenger's otorhinolaryngology : head and neck surgery [Internet]. 2019 [cited 2023 Jul 3]. Available from: https://www.worldcat.org/title/666987410 .
Mohseni M, Szymanski T. Acute Non-Traumatic Spontaneous Auricular Hematoma. 2019 Feb 16;20:204–6.
Ghat SK, Kalambe A, Maldure S. Auricular hematoma an avoidable cosmetic deformity: A chance or negligence. Am J Otolaryngol [Internet]. 2022 Jan 1 [cited 2023 Jul 3];43(1). Available from: https://pubmed.ncbi.nlm.nih.gov/34563803/
Ohlsen L, Skoog T, Sun SA. The Pathogenesis of Cauliflower Ears. An
Experimental Study in Rabbits. Scan J Plastic Reconstruction Surgery. 1975;9(1):34- 9.
Lee KJ. Infection of the Ear. In: Essential Otolaryngology Head and Neck Surgery. 8th Edition. New York: McGraw Hill, 2003; p.462-511.
McWhorter AJ, Limb CJ, Niparko JK. Otologic and Skull Base Emergencies. Emergencies of the Head and Neck. Eisele DW, McQuone SJ, editors. St. Louis: Mosby, 2000; p.367-97.
Bull TR. The Ears. Color Atlas of ENT Diagnosis. Thiem, 2003 ; p.43- 61.
Khan N, Cunning N. Pinna Perichondritis. NCBI [Internet]. 2023 Jan 2 [cited 2023 Jul 6]; Available from: https://www.ncbi.nlm.nih.gov/books/NBK572081/#article-132617.s7
Watkinson JC, Clarke RW. Scott-Brown's Otorhinolaryngology and Head and Neck Surgery, Eighth Edition: Volumes 1-3 [Internet]. 8th ed. 2018 [cited 2023 Jul 4]. 1–4360 p. Available from: https://www.worldcat.org/title/1046615713
Nasrallah F, Brewer CF, Arkoulis N, Mabvuure NT. Strategies to prevent suppurative chondritis following auricular burns: a systematic review [Internet]. 2022 [cited 2023 Jul 3]. Available from: https://www.magonlinelibrary.com/doi/10.12968/jowc.20 22.31.5.394
Rivera-Morales MD, Rodríguez-Belén JL, Vera A, Ganti L. https://www.magonlinelibrary.com/doi/10.12968/jowc.2022.31.5.394[Internet]. Cureus. 2020 [cited 2023 Jul 4]. Available from: https://pmc/articles/PMC7686808/1 .
Yoshida M, Taniguchi Y, Yoshida T, Nishikawa H, Terada Y. Ultrasonography of auricular cartilage is a potential tool for diagnosing relapsing polychondritis and monitoring disease activity. Int J Rheum Dis. 2022 Feb 1;25(2):201–9.
Ingvaldsen CA, Kim AT. Auricular Hematoma [Internet]. Norway; 2017 Jan [cited 2023 Jul 6]. Available from: https://tidsskriftet.no/en/2017/01/auricular- hematoma .
Menner AL. Disorders of the External Ear.In: A Pocket Guide to TheEar. 1st Edition. Stuttgart. Thieme, 2003;p.26-50.
Sellami M, Ghorbel A. Traumatic auricular hematoma. PAMJ [Internet]. 2017 Mar 15 [cited 2023 Jul 5];26:148. Available from: https://www.panafrican-med- journal.com/content/article/26/148/full .
Khan N, Cunning N. Pinna Perichondritis. NCBI [Internet]. 2023 Jan 2 [cited 2023 Jul 6]; Available from: https://www.ncbi.nlm.nih.gov/books/NBK572081/#article-132617.s7 .
Kroon DF, Strasnick B. Diseases of the Auricle, External Auditory Canal and Tympanic Membrane. InGlasscock Michael E, editor. Surgery of the Ear. 5th Edition. Hamilton. Ontario; p.345-67.
Yahalom S, Eliashar R. Perichondritis: A Complication of Piercing Auricular Cartilage. Postgrad. Med. J. 2003;79:29. Accessed 30 June 2020
Stroud MH. Treatment of Suppurative Perichondritis. The Laryngoscope; 88:176- 8.
Bassiouny, A. Perichondritis of Auricle. The laryngoscope 1981;91:422- 31.
Kim Y, Choi JW, Park YH. Management of an Inappropriately Treated Case of Auricular Hematoma. J Audio Auto [Internet]. 2021 Apr 10 [cited 2023 Jul
3];25(2):115–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/32829625 .
Mohamad SH, Barnes M, Jones S, Mahendran S. A new technique using fibrin glue in the management of auricular hematoma. Clin J Sport Med [Internet]. 2014 [cited 2023 Jul 3];24(6):65–7. Available from: https://pubmed.ncbi.nlm.nih.gov/24699189 .
Mohamad SH, Barnes M, Jones S, Mahendran S. A new technique using fibrin glue in the management of auricular hematoma. Clin J Sport Med [Internet]. 2014 [cited 2023 Jul 3];24(6):65–7. Available from: https://pubmed.ncbi.nlm.nih.gov/24699189/ .
Sharma A, Gnanapandithan K, Sharma K, Sharma S. Relapsing polychondritis: a review. Clin Rheumatol;2013.h. 1575-83
Kishore Prasad,S Sreedharan, Perichondritis of the auricle and its management, The Journal of Laryngology& Otology. United Kingdom; 2007;121.p.530-534.
Erez Davidi, Hava Duchman, Michal Luntz. Perichondritis of the auricle: Analysis of 114 cases(online series);2011 Available from https://pdfs.s emanticscholar.org .
Pattanaik S. Effective, Simple Treatment for Perichondritis and Pinna Haematoma. J Laryngol Otol.123(11):1246-9.
ada
Comments