CLEAR CELL CARCINOMA PAROTID
I Made Nudi Arthana
Clear cell carcinoma parotid in the head and neck area is a rare case. Clear cell carcinoma (CCC) can be found in almost all benign or malignant epithelial, mesenchymal, melanocytic or hematopoietic tumors. CCC occurs due to various factors including artifactual changes, impaired cell preservation and hydropic degeneration of organelles, or due to accumulation of glycogen, mucopolysaccharides, lipids, mucins, or phagocytosed foreign bodies in tumor cells. Clear cell changes in the tumor become more extensive as the tumor progresses or arise secondarily. All these factors make the diagnosis of clear cell difficult. Salivary gland tumors account for less than 7% of neoplasms involving the head and neck region.
LITERATURE REVIEW
Parotid Anatomy
The salivary glands are divided into major and minor salivary glands. The major salivary glands consist of a pair of parotid salivary glands, submandibular salivary glands and sublingual salivary glands, while the minor salivary glands are spread throughout the oral cavity in the hundreds. 1
The parotid salivary gland is the largest major salivary gland, weighing about 14-18 grams and measuring approximately 6x4 cm, which is located just anterior and inferior to the auricle. The parotid salivary gland is covered by the parotid fascia which is a continuation of the superficial layer of the deep cervical fascia. The superficial layer of the parotid fascia is continuous with the surrounding muscles, anteriorly to the masseter muscle, behind to the sternocleidomastoid muscle. And in superior to direction zygoma. Layer This Also forms septa into the parotid salivary gland. The deep layer of the parotid fascia separates the parotid salivary gland from the submandibular salivary gland, where it extends toward the mandible anteriorly, toward the styloid process posteriorly, and towards the stylomandibular ligament inferiorly. 1,2
The duct of the parotid salivary gland (Stensen's duct) is 4-6 cm long, begins from the anterior part of the parotid salivary gland and runs horizontally to the masseter muscle approximately 1.5 cm below the zygoma. At the anterior border of the masseter muscle, the duct turns medially and passes through the cheek cavity into the oral cavity. mouth through papilla small in across the teeth molar second. 12.13 Vessels primary blood Which supply gland saliva parotid is artery carotid external. Artery it's running in a way parallel with OS mandible Then branching become artery maxillary and superficial temporal arteries. A branch of the superficial temporal artery, the transverse facial artery, supplies the parotid salivary gland, Stensen's duct, and the masseter muscle. 2,3,4
Parotid salivary gland drainage is through the posterior facial vein, which is a union of the superficial temporal vein and the maxillary vein. This vein runs beneath the facial nerve and lateral to the carotid artery. This vein then joins the postauricular vein to form the external jugular vein. The posterior facial vein can also join the anterior facial vein to form the common facial vein, which then empties into the internal jugular vein. 1,4
The parotid salivary glands are closely related to the important structures around them, namely vein jugular internal, artery carotid external along with its branches, gland lymph, auriculotemporal branch of the trigeminal nerve and the facial nerve. 1 The facial nerve divides the parotid salivary gland into two parts, namely the majority of the gland lies superficial to the facial nerve, while a small part lies deep and medial to the facial nerve. The facial nerve exits the temporal bone at the stylomastoid foramen, which is located at the junction of the mastoid process and the base of the styloid process. When the nerve enters the parotid salivary gland, it will be divided into two parts, namely the temporo-facial part towards the top and the cervico-facial part towards the bottom. Based on this division, five different areas of the face are innervated by the nerves: (1) The temporal branch that crosses the zygomatic arch to the temporal area; (2) The zygomatic branch to the lateral angle of the eye; (3) The buccal branch that goes to the nose and mouth; (4) The mandibular branch which innervates the muscles of the lower lip and chin; (5) The cervical branch which goes to the neck platysma. 1,3,4
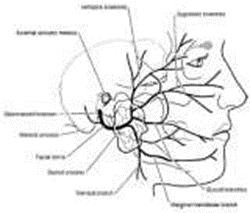
Picture 1 . Gland parotid And branching facial nerve
Histologically, the parotid salivary glands are mostly composed of acinar gland cells connected to the salivary duct. This structure is located in a glandular mesenchymal tissue consisting of connective tissue, blood vessels and lymphatics, lymphatic tissue and nerve fibers. 2,3
Gland acinus is manufacturer main saliva, Which bring enzyme such as amylase, and sialomucin. The acinar glands contain myoepithelial cells that form a spider-web-like structure and function in the process of emptying saliva production with contractile movements. 3.4 The salivary glands constantly continue to produce a certain amount of saliva, even when the body is resting. In the parotid salivary glands, the amount of secretion when stimulated can reach 4-5 times more than secretion when resting. 2.4 The total amount of saliva production from all salivary glands is 500-1000 milliliters per day. 2.3 Saliva own a number of important functions, among others others lubricate the food bolus and protect the surface of the oral cavity with a biofilm membrane; maintain the oral cavity milieu with a pH ranging between; maintain the integrity of the teeth; antimicrobial effects with the content of IgA, IgG, IgM, protein, mucin, peptide and enzyme components; and help the process of taste and digestion. 1,4
Definition
Primary salivary gland clear cell neoplasms can be divided into those that require diagnostic evidence of myoepithelial differentiation (eg, clear cell myoepithelial carcinoma (CCMEC) and epithelial-myoepithelial carcinoma (EMEC)) and those that do not (eg, CCC). Most of these tumors are reported as sporadic cases with the exception of a few cases in which myoepithelial differentiation has not been documented. on CCC. According to definition, CCC contain clear cell in proportion significant, but not included in other neoplastic entities. Although non-lipid And non-mucin, However tumor clear cell rich glycogen in salivary glands long recognized, they have recently been included in the WHO classification as carcinomas degrees low. Classification WHO tumor gland saliva No defined a specific category for clear cell tumors and simply stated that the presence of clear cells is a common feature of neoplasms originating from that location. 5,7 These tumors were previously referred to as monomorphic variant of EMEC, mucin-depleted mucoepidermoid carcinoma , and myoepithelial carcinoma. CCC is separated from these diseases because of the lack of squamous, mucinous, or myoepithelial differentiation.
Type Tumor Parotid
Salivary gland tumors account for 2%-6.5% of all tumors in the head and neck. neck. 80% tumor gland saliva there is on gland saliva parotid, 10%-15% in the submandibular salivary glands, the rest in the sublingual salivary glands and minor salivary glands. The rule of thumb that needs to be remembered is the "rule of 80", where 80% of all salivary gland tumors occur in the parotid, 80% of parotid tumors are benign, and 80% of benign parotid tumors are pleiomorphic adenomas. Warthin's tumor is the second most common benign lesion. The most common malignant tumor is mucoepidermoid carcinoma. 7,8
Table 1 . Incident Tumor Gland Saliva Parotid Based on Type Tumor. 8
Type Tumor | Incident (%) |
Pleomorphic adenoma | 53.3 |
Warthin's tumor | 28.3 |
Other benign tumors | 3.8 |
Total tumor benign | 85.4 |
Mucoepidermoid carcinoma | 9 |
Adenocarcinoma | 1.5 |
Squamous cell carcinoma | 0.9 |
Acinic cell carcinoma | 0.9 |
Malignant mixedtumor | 0.9 |
Adenoid cystic carcinoma | 0.5 |
Tumor malignant other | 0.9 |
Total tumor malignant | 14.6 |
Etiopathogenesis
There are two main theories as to how salivary gland tumors arise, but the consensus is that each form of tumor arises from a specific differentiated cell origin within the salivary gland unit. Excretory stem cells develop into mucoepidermoid and squamous cell carcinomas, while intercalated stem cells can develop into pleomorphic adenomas, adenoid cystic carcinomas, oncocytomas, adenocarcinomas, and acinic cell carcinomas. Several factors are thought to play a role, including genetics, ionizing radiation, chemical exposure. Radiation exposure has also been associated with parotid carcinoma 15 years after the event. Smoking and alcohol consumption have been associated with head and neck squamous cell carcinoma, and scalp and neck skin malignancies have also been known to metastasize to the parotid gland. Some have linked occupational exposure to silica dust, nitroasmine, and other chemicals. It has been suggested that smoking and alcohol consumption are not associated with salivary gland tumors, except for Warthin's tumor. 4 Antonescu et al recently found consistent ESWR-ATF1 fusion in HCCC, which was not found in other salivary gland tumors containing clear cells. There is a clear resemblance between HCCC clear cell nests and stromal hyalinization and features similar to some cases of soft tissue myoepithelial tumors. 5
Epidemiology
Salivary gland tumors account for 2%-6.5% of all tumors in the head and neck. and neck. 80% of salivary gland tumors are found in the parotid salivary glands. CCC is a low-grade malignant neoplasm that represents about 1% of all salivary gland tumors. This tumor is more common in women with an average age of 50-60 years. Malignant neoplasms make up 15-35% of all parotid gland tumors; 21-42% of them occur as a result of the process metastatic. Most metastatic salivary gland tumors originate from lesions in the head and neck area, consisting of melanoma in 45% of cases and squamous cell carcinoma in 45% of cases. skin on 37%. Only part small Which originate from location Which far as the lungs, breasts, kidneys, gastrointestinal tract, and prostate. 3 From the literature during 50 last year, found 35 report renal case cell metastatic carcinoma (RCC) to the parotid gland. Age of diagnosis ranges from 40 to 83 years. Metastatic RCC is more common in men, in accordance with the male predominance of RCC in general. 6
Histopathology
Histologically, the appearance of HCCC is very variable. Clear cell predominance is seen in only a minority of cases and the tumor cells often have clear or mixed eosinophilic cytoplasm (Fig. 1a). Tumors without clear cells may be seen but generally they have the same growth pattern as typical HCCC (Fig. 1b), i.e. the cells are arranged in small nests, long and short cords, thin interconnected trabecular structures and single cells. There is a tendency for the cells to be in the center of the mass surrounded by a hyalinized basement membrane-like material (Fig. 1c). These are often sharply demarcated from the desmoplastic or fibrocellular stroma and may occasionally appear myxoid and resemble a pleomorphic adenoma. Juxtaposition of these two types within the tumor is pathognomonic for the diagnosis of HCCC. The presence of cribriform hyalinized stroma may also mimic other more common salivary gland tumors, especially in cases with few clear cells (Fig. 1d). 5
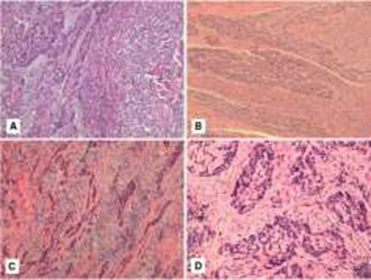
Fig. 2 a–d Typical examples of HCCC showing a combination of cords and nests of clear and eosinophilic cells in a hyalinized background (a). Some HCCCs show areas without obvious clearing but show a similar growth pattern. Case This Also show invasion perineural Which prominent (b). The existence of stroma. Fibrocellular overlying hyalinized stroma is a common finding (c). Hyalinization may resemble cribriform growth (d). 2
Tumor cells at the edge or periphery of the mass have a higher tendency to form nests and extensive infiltration without stromal deposits or desmoplastic response. Some may also appear as short thin cords between skeletal muscle fibers and may be very difficult to see with H&E (Fig. 2a). Faint nests are more obvious on immunohistochemical staining. HCCC is often associated with the surface mucosal epithelium either as an abrupt or single-cell pagetoid-like growth. It may also be accompanied by pseudoepitheliomatous hyperplasia of the epithelium. This is seen in 44% of cases in the oral cavity (Fig. 2b). Focal squamous differentiation of tumor nests is also occasionally seen (Fig. 2c). Perineural invasion (PNI) and intraneural invasion are common and occur in almost half of the cases (Fig. 1b). Other focal findings include the formation of native ducts or, in most cases, entrapment of ducts (Fig. 2d). This is particularly common in parotid CCC. Individual cells are small and plain with atypia. minimal. Some ''rachinoid'' or ''popcorn'' nuclear membrane irregularities may be seen, as may pseudonuclear inclusions, but nuclear size shows minimal variation (Fig. 3a). 7
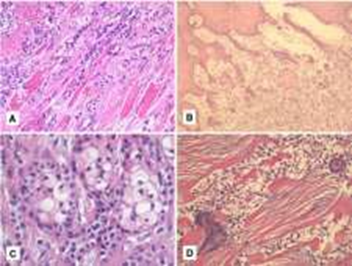
Fig. 3 a–d Skeletal muscle infiltration is common and sometimes subtle (a) Nearly half from example HCCC cavity mouth relate to epithelium surface
(b). Sometimes squamous differentiation can be seen (c). True ductal differentiation is rare. Trapped ducts are more often seen especially in the parotid case (d). 2
Multivacuolated or pseudosebaceous cells may be seen. Mitotic figures are rare and amount <1 per 10 LPB only on a number of case appear only until 5 per 10 LPB. 5 Small nucleoli. Necrosis is generally not seen. Mucinous cells may occasionally be present, but close examination with the mucicarmine special stain shows dot-like mucin or real intracellular mucin in most cases (Fig. 3b). 7 Clear cells show positive granular PAS and diastase sensitivity, indicative of glycogen in the cytoplasm. This stain also highlights the hyalinized stroma . Congo red stain is negative, although the stroma appears similar with amyloid. HCCC No own growth papillary, chondroid stroma or cystic clefts lined with goblet cells. When present, small cystic clefts are generally lined by typical clear cells rather than mucinous cells (Fig. 3c). 2

Fig. 4 a–d Most HCCCs show minimal atypia with small, plain nuclei (a). Mucinous differentiation is seen in nearly half of the cases, usually focal but may be diffuse (b). Rarely, small cystic clefts may be seen but are not lined by mucinous cells (c). Virtually all cases are positive for p63 and/or HMWK (d). 2
Symptom And Sign Clinical
Most HCCCs arise as masses in the oral cavity and are assumed to arise from minor salivary glands. A small number of cases may arise from major salivary glands, nasopharyngeal or laryngeal tumors. Minor salivary glands are involved in two-thirds of cases according to AFIP. The tumors are usually submucosal, usually presenting as edema and occasionally ulcerating. Signs and symptoms of invasion nerve cranial sometimes happen. Although it is said own pause time long, most patients immediately have a short history of complaints before look for help medical. Journey experience nature Indolent And mass is generally painless. CCC is not very aggressive and grows very slowly so it is often asymptomatic, so the tumor often reaches a fairly large size before it can be diagnosed. 3 These lesions are often found on routine dental examinations and many are biopsied and examined first by an oral surgeon or pathologist. Macroscopically, these carcinomas appear solid, gray with a rubbery consistency. 8 Tumors range in size from 1.0 to 4.5 cm (mean 2.0–3.0 cm) with a white-brown transverse surface macroscopically. Cystic changes are uncommon. HCCC may appear relatively well-circumscribed but is not encapsulated and has a tendency to infiltrate surrounding tissue, despite the macroscopic circumscribed appearance . 2
Diagnosis
The diagnosis of parotid CCC is based on anamnesis, physical examination, supporting examinations such as radiology and histopathology. From the anamnesis, it was found that parotid CCC generally grows slowly indolently, without pain. Detected incidentally during routine examination or after the lump in the parotid area enlarges. Tumors are generally submucosal, usually appear as edema and sometimes become ulcers. Signs and symptoms of cranial nerve invasion sometimes occur. 1,2
On inspection physique generally found tumor shaped round in parotid area with a flat surface and a firm, elastic consistency. The size of the tumor ranging from 1.0 to 4.5 cm (average 2.0–3.0 cm) with a white-brown transverse surface macroscopically. Cystic changes are not commonly seen. 1,2 Fine Needle Aspiration Cytology ( FNAC ) is a relatively simple, safe, and reliable examination method. quite accurate and cheap in diagnosing glandular neoplasms spit.1.6 Sensitivity FNAC in differentiate tumor benign And malignant gland saliva range between 85.5%-99% And its specificity range between 96.3%-100%, as well as results interpretation cytology Which fast Also is important thing use prevent action invasive others. 1,2,6 However accuracy FNAC also depends on the experience and skills of the pathologist. 1,18 Open biopsy on tumor gland saliva parotid must avoided Because at risk to injure facial nerve. 1,18 Open biopsy is rarely performed and is only performed in cases that are clearly malignant and in cases where FNAC cannot be diagnosed. In this case, open biopsy aims for histopathological diagnosis and selection of the most appropriate palliative therapy. 1
Various modalities are used in imaging of glandular tumors. saliva. These include Computed Tomography Scan ( CT Scan ) and Magnetic Resonance Imaging ( MRI ), which are the modalities of choice in diagnosing and determining tumor extension. 1,19,20 CT Scan and MRI examinations cannot distinguish whether a tumor is benign or malignant, but both can show tumor infiltration and extension. 1,20
In cases of predominantly clear cell, a definitive diagnosis may be difficult because many of these tumors have similar histologic features. The histopathologic finding of malignant clear cell tumor in a parotidectomy specimen requires consideration of the differential diagnosis between primary and metastatic parotid clear cell tumor. Carcinomas of the kidney, liver, colon, prostate, and thyroid are known to have the potential to experience differentiation clear cell And everything capable metastasize to the maxillofacial area especially renal cell carcinoma (RCC). 3
Salivary gland CCCs typically express epithelial markers (cytokeratins, EMA, and CEA) but lack myoepithelial markers (S-100 protein, actin, vimentin, and glial fibrillary acidic protein). Immunohistochemical staining of adenocarcinoma RCCs shows negativity for high-molecular-weight cytokeratins and patchy weak-to-moderate staining for low-molecular-weight cytokeratins (CAM 5.2) in more than 80% of cases. They also stain strongly for EMA and vimentin and are negative for actin, S-100, glial fibrillary acidic protein, and CEA. Recently, CD10 immunoreactivity has been shown in 90% to 94% of RCCs, increasing the specificity of the histopathologic diagnosis. CD10 is a natural endopeptidase associated with cell membranes, called enkephalinase, CALLA, and EC3.3.24.11, and plays an important physiological role in degrading active peptides, including those involved in autocrine growth stimulation of certain cancers. 3
Ewing sarcoma breakpoint region 1 (EWSR1) rearrangement and EWSR-ATF fusion have been described in HCCC. It has been reported that 87% of HCCC show EWSR1 rearrangement . Because EWSR-ATF fusion is specific for HCCC, it can be assessed by RT-PCR, so EWSR1-ATF fusion and EWSR1 rearrangement can be used as markers for HCCC to distinguish it from other salivary gland neoplasms. 9 HCCC commonly has EWSR1 gene translocations that cause EWSR1-ATF fusions. 10 Although this can be demonstrated by EWSR1 FISH, given that odontogenic CCC also has this translocation (and a small proportion of MEC also have EWSR1-POU5F1 translocations), confirmation of EWSR1 binding pairs by FISH or NGS may be considered for diagnostic confirmation. 11,12
In cases where definitive tumor classification cannot be made with standard cytology and/or routine H&E cell block specimens, additional tests may be helpful in differentiating between the following entities (Table 1). Based on staining characteristics, an algorithmic approach to salivary gland clear cell lesions with several immunohistochemical stains has been proposed: pancytokeratin, vimentin, calponin, and p63 (Fig. 4). Because parotid metastases often originate from the skin, melanoma need to be considered on the lesion clear cell gland unspecified saliva; mixed pancytokeratin immunohistochemistry (eg, AE1/AE3/Cam5.2) helps exclude melanoma (negative). For pancytokeratin-positive lesions, vimentin immunohistochemistry can help separate acinic cell carcinoma, clear cell carcinoma, and MEC (negative) from neoplasms For these tumors, p63 immunohistochemistry differentiates primary CCC (positive) and MEC (positive in epidermoid cells) of acinic cell carcinoma (negative). 6
Table 2. Immunohistochemistry And coloring special from lesi clear cell gland saliva. 6

Diagnosis Appeal
Generally, diagnosis appeal clear cell tumor parotid mainly is a variant clear cell from primary tumors such as myoepithelial clear cell carcinoma, EMEC, acinic clear cell carcinoma, salivary gland clear cell adenocarcinoma and hyalinizing CCC (also called primary CCC). In addition, mucoepidermoid clear cell carcinoma, clear cell oncocytoma and odontogenic clear cell tumors also need to be excluded. Immunohistochemical evaluation is important to differentiate these tumors. Some consider that differentiating CCC from metastatic salivary gland adenocarcinoma RCC is almost impossible by pathology alone and requires clinical evaluation to rule out primary renal tumors.7
Cytology samples of oncocytomas are usually highly cellular, containing sheets of or trabeculae of large polygonal cells with granular cytoplasm, sharp cell borders, small, round central nuclei, and prominent cherry-red nucleoli. Well-differentiated acinic cell carcinoma may have an appearance similar to oncocytoma; however, acinic cell carcinoma lacks prominent nucleoli and typically forms loosely cohesive acinar-like clusters (rather than sheets or trabeculae). Acinic cell carcinoma may be associated with a dense lymphoid infiltrate containing prominent germinal centers, but mitoses and necrosis are uncommon. 15
MECs have diverse cytomorphology and consist of at least four types. cell malignant—cells mucin-producer (goblet), cell intermediate, cell squamous (epidermoid), And clear cells— distribution relatively varies according to histological grade of the tumor. Mucin-producing cells are medium to large in size. big with eccentric nuclei and vacuolated cytoplasm. Intermediate cells vary from small, basaloid-type to medium-sized, cuboidal-type and show varying degrees of polymorphism depending on the histologic grade of MEC. Squamous cells have the appearance of mature squamous epithelial cells. Clear cells are large, round cells with clear cytoplasm and small nuclei and nucleoli. Low-grade MEC often appears as a paucicellular, polymorphic lesion, with mucus-producing cells predominating and relatively few intermediate and squamous cells; these features are nonspecific and may be difficult to distinguish from benign lesions, such as mucoceles. Intermediate-grade MEC is more cellular than low-grade MEC and has intermediate and squamous cells predominating; mucus-producing cells are common, but clear cells are rare. High-grade MEC consists almost entirely of loosely cohesive pleiomorphic cells, with focal areas of mucus-producing and intermediate cells; the presence of these cell types in high-grade salivary gland lesions suggests the diagnosis of MEC. 11 Table 2 summarizes the immunohistochemical staining patterns of clear cell tumors in the differential diagnosis of HCCC. 18
Table 3. Diagnosis appeal And pattern coloring tumor clear cell head and neck. 18

Management
Management of CCC is Wide excision of the tumor performed with parotidectomy, this operation is the first choice for most CCC, although neck dissection and radiotherapy are also performed in some cases. Excision can also be performed via a transcervical or intraoral approach. The decision to include lymph node dissection or radiotherapy is generally based on the presence of positive margins, high-grade histology, invasion (vascular/neural) or neck lymph nodes. positive. When detected metastasis KGB or under consideration Possible
occurs based on clinical or radiographic examination, partial or modified neck dissection can be performed. Although these prognostic factors also apply to CCC, an additional factor associated with lymph node metastasis is the presence of mitotic activity. 3 Many cases receive postoperative radiotherapy; however, there is no standard management of this tumor because it is rare and responds well in most cases. 6,19
In their study, Solar et al. observed that HCCC can exhibit aggressive behavior, especially related to cervical lymph node metastasis. 20 They recommend a thorough neck examination when treating patients. diagnosed with HCCC and neck dissection should be considered if there is a potential locoregional risk. Surgical reconstruction is required in some cases, and oral and oropharyngeal defects are reconstructed with soft tissue flaps obtained from the neck, cheek, or soft palate. Postoperative radiotherapy is recommended if surgical margins are positive or the lesion is aggressive. This has been shown to improve locoregional control in salivary gland tumors. malignant in general. On the other hand, chemotherapy is generally considered ineffective. 19
In comparison, metastatic RCCC does not respond well to radiation therapy and its role is still debated. Therapy with interleukin-2, interferon alpha and 5-f fluorouracil may be useful in cases of residual disease after resection, although partial responses are less than 25%. 11
Complications
Complications vary from multiple recurrences to local nodes or distant sites. Patients may experience multiple recurrences up to two decades after resection. and tends to occur in intraoral locations (65%). The recurrence rate is 17% and the metastatic rate is 21%. Therefore, it is important to do follow-up. 7
Parotidectomy surgery can cause complications in the form of facial nerve paralysis and Frey syndrome. Facial nerve paralysis can occur partially or completely, and can affect certain branches or all branches of the facial nerve. Temporary facial nerve paralysis occurs in 10%-30% of patients after the operation. parotidectomy. 8 Stimulation Which excessive can result in damage and paralysis of the nerve that is temporary and can disappear in a few weeks to a few months. 7 Permanent facial nerve paralysis occurs in less than 3% of patients after parotidectomy. 5 Permanent paralysis occurs when the nerve is cut during surgery due to tumor invasion. 7,8 The incidence of facial nerve paralysis is more common in patients who undergo total parotidectomy than in patients after superficial parotidectomy. 5 The incidence of facial nerve disorders is reported to increase in tumor treatment operations that recurrent . 6 Frey syndrome, also called gustatory sweating , can occur after parotidectomy. This is thought to be due to cross-reinnervation of the autonomic pathways. to the parotid salivary glands so that the parasympathetic fibers stimulated by smell and taste, innervate the sweat glands and blood vessels. As a result, sweat and redness occur around the skin in the parotid region when chewing. 7 Frey syndrome is found in about 10% of patients after parotidectomy. 8
Prognosis
Most patients with HCCC have a good prognosis. In one study. This tumor has a tendency for locoregional recurrence in 12–17% of cases and can occur with lymph node metastasis or distant metastasis. Solar et al reported a lymph node positivity rate of 25%; however, this is different from another larger series by Weinreb where no lymph node metastasis or distant metastasis was found with a follow-up of 48 months. Overall, the prognosis of parotid CCC is relatively good. 6
REFERENCE
Strong BC, Johns ME, Johns MM. Anatomy and Physiology of the Salivary Glands. In: Bailey BJ, Johnson JT, Newlands SD, editors. Head & Neck Surgery- Otolaryngology. 4th Edition. Philadelphia: Lippincott Williams & Wilkins; 2006. p.517- 25.
Probst R, Grever G, Iro H. The Salivary Glands. In: Basic Otorhinolaryngology : A Step by Step Learning Guide. 2nd Edition. New York: Georg Thieme Verlag; 2006. p.131 41.
Lee KJ. The Salivary Glands: Benign and Malignant Diseases. In: Essential Otolaryngology. 8th Edition. New York: McGraw-Hill Companies, Inc.; 2003. p.535-45.
Adams GL. Diseases of the Salivary Glands. In: Boies Fundamentals of Otolaryngology : A Textbook of Ear, Nose, and Throat Diseases. 6th ed. Philadelphia: WB Saunders; 1997. p.305-7.
Said-Al-Naief N, Klein MJ. Clear Cell Entities of the Head and Neck: A Selective Review of Clear Cell Tumors of the Salivary Glands. Head Neck Pathol. 2008 Jun;2(2):111–5.
Weinreb I. Hyalinizing Clear Cell Carcinoma of Salivary Gland: A Reviews and Updates. Head Neck Pathol. 2013 Jul;7(S1):20–9.
Rodríguez MS, Reija MFG, Rodilla IG. Primary clear cell carcinoma of parotid gland: Case report and review of literature. J Oral Maxillofac Pathol JOMFP. 2013;17(1):101– 5.
Eisele DW. Salivary Gland Neoplasms. In: Bailey BJ, Johnson JT, Newlands SD, editors. Head & Neck Surgery-Otolaryngology. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2006. pp. 1515-32.
Alvi S, Chudek D, Limaiem F. Parotid Cancer. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Oct 31]. Available from: http://www.ncbi.nlm.nih.gov/books/NB K538340/
Hellquist H, Skalova (auth.) A. Histopathology of the Salivary Glands [Internet]. 1st ed. Springer-Verlag Berlin Heidelberg; 2014 [cited 2023 Oct 31]. Available from: http://gen.lib.rus.ec/boo k/index.php?md5=c4301de7f8f275227fadfe7e11098e36
Udager AM, Rungta SA. Metastatic renal cell carcinoma, clear cell type, of the parotid gland: A case report, review of literature, and proposed algorithmic approach to clear salivary gland cell neoplasms in fine‐needle aspiration biopsies. Cytopathol Diagn. 2014 Nov;42(11):974–83.
Antonescu CR, Katabi N, Zhang L, Sung YS, Seethala RR, Jordan RC, et al. EWSR1- ATF1 fusion is a novel and consistent finding in hyalinizing clear-cell carcinoma of salivary gland. Genes Chromosomes Cancer. 2011 Jul;50(7):559–70.
Daniele L, N ikolarakos D, Keenan J, Schaefer N, Lam AK yin. clear cell carcinoma, not otherwise specified/hyalinizing clear cell carcinoma of the salivary gland: The current nomenclature, clinical/pathological characteristics and management. Crit Rev Oncol Hematol. 2016 Jun;102:55–64.
Yamanishi T, Kutsuma K, Masuyama K. A Case of Hyalinizing Clear Cell Carcinoma, So-Called Clear Cell Carcinoma, Not Otherwise Specified, of the Minor Salivary Glands of the Buccal Mucosa. Case Rep. Otolaryngol. 2015 Oct 27;2015:e471693.
Zhao Y nuo, Wang X, Liang F hua, Zhang W jie, Song X tao. Hyalinizing clear cell carcinoma of salivary glands: A retrospective study focused on uncommon morphology, immunohistochemistry, and detection of gene fusion using fluorescence in situ hybridization. Pathol - Res Pract. 2018 Mar;214(3):380–4.
Moutasim KA, Thomas GJ. Salivary gland tumors: update on molecular diagnostics. Histopathol Diagn. 2020 Apr 1;26(4):159–64.
Badawy W, Abdelfattah AS, Sallam HA. Activating Transcription Factor 1 (ATF1) Immunohistochemical Marker Distinguished HCCC from MEC. J Mol Pathol. 2023 Sep;4(3):178–88.
O'Sullivan-Mejia ED, Massey HD, Faquin WC, Powers CN. Hyalinizing Clear Cell Carcinoma: Report of Eight Cases and a Review of Literature. Head Neck Pathol. 2009 Sep;3(3):179–85.
Kauzman A, Tabet JC, Stiharu TI. Hyalinizing clear cell carcinoma: A case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontology. 2011 Jul;112(1):e26–34.
Solar AA, Schmidt BL, Jordan RCK. Hyalinizing Clear Cell Carcinoma. Cancer. 2009 Jan 1;115(1):75–83.
Gudelj G, Simunjak T, Zizic M, Simunjak B, Jurlina M. An unusual case of hyalinizing clear cell carcinoma in a sinonasal cavity and cranial base. J Surg Case Rep. 2020 Oct 27;2020(10):rjaa436.
Comments