Closed Reduction
I Made Nudi Arthana
Closed Reduction for Fracture OS Nasal
Management options for Os fractures Nsal can be with closed reduction or open reduction considering the type and severity of the fracture. The best time for proper and most accurate management is done immediately after injury, before there is significant tissue edema. The goal of management is to restore appearance, restore airway patency, midline septum, maintain nasal valve integrity, prevent postoperative complications such as stenosis, septal perforation, columella retraction, and saddle deformity or persistent deformity.
Literatur Review
Operative
Deformity due to nasal bone fracture is often encountered and requires reduction. with fixation adequate to fix nasal position. Handling of simple nasal bone fractures can be done by repositioning the fracture under local anesthesia. If bleeding occurs Keep going ongoing, nose must closed with gauze tape Vaseline for 48 hours. If possible, the bone fragments should be repositioned within a few hours before swelling occurs which will cause deformity. External splints are used to maintain the position of the nasal bones. If splints are not used, deformity is likely to occur. 13,26,29
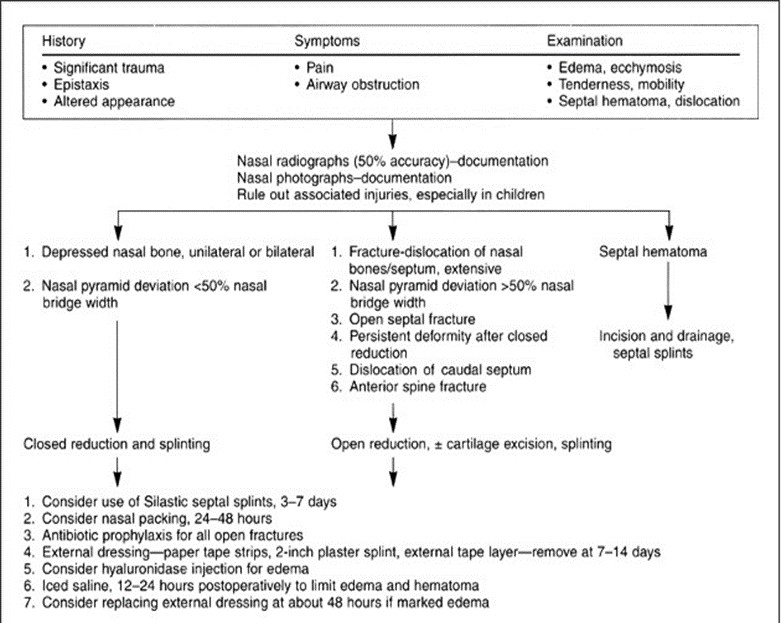
Chart 2. Handling trauma nose 3
Splint fracture OS nasal simple describe splint nose perfect as a piece of soft metal plate (size 22) shaped like an hourglass. So the bottom in accordance with the shape of the nose and parts on from the plate is on the forehead. Splint nose This is splint normal Which can to form nose and evens out the pressure on all sides, then held in place by a T-shaped adhesive plaster. across forehead in part on And plaster in part lower withhold nose. Only moderate pressure can be used and the bandage cannot be removed for a long period of time. time minimum two days. Limit time the use of medication is until the nose is not inflamed and swollen. 23
The closed reduction manipulation technique is a technique used to reduce a newly occurring nasal bone fracture. Approximately 2-3 weeks after the trauma, it will form network fibrotic on fragment bone in position Which No should And this is it Which cause reduction with technique This No Possible done. In
nasal bone reduction action, some tools that can be used such as blunt elevators ( Boies Nasal Fracture Elevator ), Asch forceps , Walsham forceps , short nasal speculum, Killian long speculum and bayonet tweezers. Nasal bone fractures can be reduced with forceps Walsham Which have distance between eye knife And cover section, Where part the allow closing network nose Which not destroyed. 10,21,26

Picture 11. Walsham forceps , Boies elevator , Ash forceps , nasal speculum, nasal suction , bayonet forceps.
Eye knife Walsham forceps which wide rather grooved to achieve the outer wall of the nose and protects nasal skin. The inner blade is smaller and shaped to reach the inner nose. 23,26
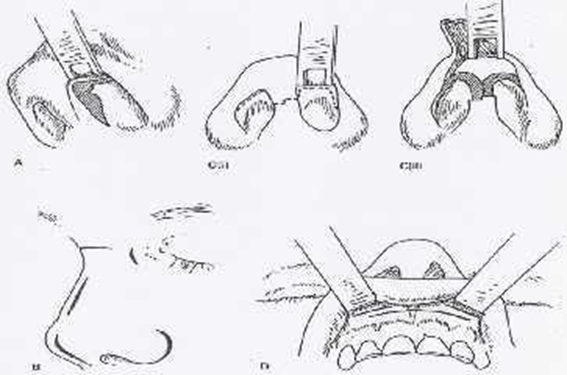
Doctor expert surgery must be careful in determine location from line fracture and it is very important not to use Walsham forceps in above the fracture line for move second process nasofrontalis. However forceps Walsham can be used For move second process nasal go out maxilla and use controlled force to avoid sudden jerking movements. To reposition the nasal bones, the septum is then grasped with Asch forceps. Which placed in behind back rice, manipulation septum nasal using Asch forceps to straighten the nasal septum. Forceps This was created on the same principle as forceps Walsham , but forceps Ash have eye knife Which can hold septum, Where part eye knife the separated from handle main part lower with size more big And curve Which useful For avoid the occurrence of severe or more extensive compression and damage to the columella. 23,26

Picture 12. Reduction closed with use forceps Asch
Reposition open under consideration For done when 1) has happen septal fracture open, 2) fracture dislocation wide bone nose And septum nasal, 3) the occurrence of caudal septal fracture dislocation, 4) pyramid deviation of more than half the width of the nasal bridge, 5) permanent changes in shape after closed repositioning, 6) Because reposition change form septum Which No adequate, 7) occurrence of hematoma septum, 8) combination of changes form septum and alar cartilage, as well as 9) the occurrence fracture displacement spine rice front And existence history intranasal surgery . 2.27
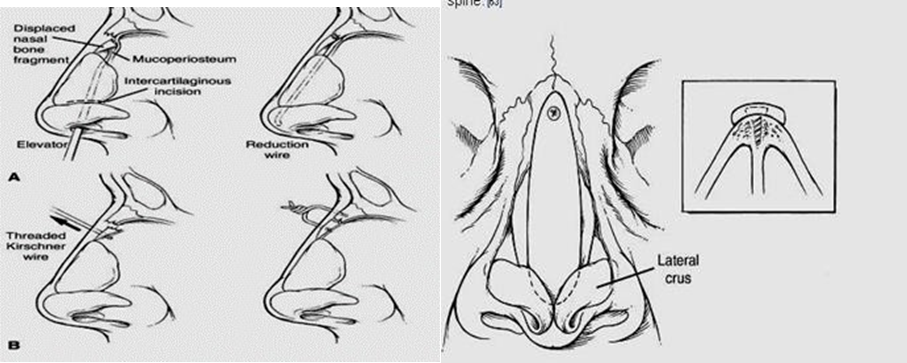
Picture 13 . Technique incision with reduction open on fracture OS nasal.16
Reposition open done If must do reposition part nasal pyramid consequence fracture occurrence bone nasal And bone vulnerable septum nasal Which interrelated. The septum can be reached through a hemitransfixion incision on the dislocated side, then the nasal bone fracture line can be reached through bilateral intercartilage incisions. The dorsal skin raised in above the lateral cartilage top and periosteum nasal bone is removed. 20 Another technique uses an intranasal approach through an incision. intercartilaginous For reduce depression broken bone nose. After surgery mucoperiosteal tunnel segment lower, wire placed in distal part below the root of the nose stable and lower distal lateral cartilage For guard fragment Which elevated. Wire cut And piece small left in cavity rice to enable retrieval after 10 to 14 days. The success rate of action with this method is reported to be 85%. 16
Complications
Complications of nasal bone fractures are divided into early complications and late complications .
Immediate Complications( early )
Immediate complications are temporary, including edema, ecchymosis, epistaxis, hematoma, infection and liquor leakage. Generally resolve spontaneously but hematoma requires drainage. Septal hematoma in every case of septal trauma must be evacuated, because it can cause infection which can occur necrosis bone vulnerable septum And Finally formed deformity saddle. Hematoma septum must suspected If got painful And swelling Which persists, this complication needs to be considered in children. A silastic splint can be used to prevent re-accumulation of blood at the hematoma site. 3,28,30
The presence of epistaxis can heal spontaneously, but if necessary, cauterization, anterior or posterior nasal tampons or ligation of blood vessels can be performed. Bleeding from the anterior side is usually due to laceration of the anterior ethmoid artery, a branch of the ophthalmic artery. Bleeding from the posterior side comes from the posterior ethmoid artery or the lateral nasal branch of the sphenopalatine artery, if necessary, ligation of the internal maxillary artery. 28,30
Prophylactic antibiotics should be given to patients with chronic weakness and with septal or dorsal hematoma. If there is a cerebrospinal fluid leak due to a fracture of the cribriform plate or posterior wall of the frontal sinus, it will usually close spontaneously with 4-6 weeks of observation. 30
Complications Slow ( late )
Airway obstruction, secondary deformities, adhesions, fibrosis (formation of network tie) or contracture (shortening) network muscle nasal), saddle nose, and septal perforation are late complications of nasal fractures. Complications This should can prevented more beginning, disproportion nasofacial can occurs with the formation of a long nose especially during puberty. In addition, it can occur obstruction duct nasolacrimalis which causes epiphora, thing This can be diagnosed radiologically by inserting contrast through the inferior punctum. The part of the duct above the blockage will appear widened. Once the location of the blockage is known, a new channel can be created connecting the lacrimal sac with the inferior meatus using polyethylene pipe, this action called dacryotic rhinotomy. 3,28,30
REFERENCE
Donald PD, Sykes J. Facial Fracture. In: Ballenger JJ, Snow JB. Ballenger's Otolaryngology Head and Neck Surgery. 6th ed. Hamilton: BC Decker Inc; 2003. p.900-46.
Michael F Zide. Nasal and Nasoorbital Ethmoid Fractures. In: Dina KR, Delois P, Darlene BC, editors. Principles of Oral and Maxillofacial Surgery. Philadelphia: Lippincott; 1992. p. 547-57.
Grant S, Carlos M. Nasal Fracture. In: Byron J Bailey, et a. Otolaryngology Head and Neck Surgery. Philadelphia; Lippincott Williams & Wilkins: 4th ed . 2006. 71A. p996-1008.
Tardy ME. Surgical Correction of Facial Deformities. In Ballenger JJ. Diseases of the Ear, Nose, Throat, Head And Neck. Translation Staff Expert Part ENT RSCM-FKUI. Jakarta: Binarupa Aksara. 1994. p.28-99.
Walsh WE, Korn RC. Sinonasal Anatomy, Function, And Evaluation. In: Bailey BJ, Johnson JT. Head and Neck Surgery-Otolaryngology. 4th ed, Vol.1. Philadelphia: Lippincott Williams & Wilkins; 2006. p.307-19.
Weller MD, Drake AB. A Reviews of Nasal Trauma. Brit Med J . London. 2006; 8
: 21-8. (accessed date 22 May 2015). Downloaded from http://www.amedeo.co.id
Ballenger JJ. Anatomy and Physiology Of The Nose And Paranasal Sinuses. In: Ballenger JJ, Snow JB. Ballenger's Otorhinolaryngology Head And Neck Surgery.6th ed. Hamilton: BC Decker Inc; 2003. p.547-60.
Ross Adam T, Nasal and Septum Frakturs.2013. (accessed 21 July 2015) Downloaded from http://emedicine. medscape.com/article/878595-overview#showall.
Mountain Roudney E. Surgical Correction of Nasal Fracture. Bleach Nigel et all. In Operative Otorhino-Laryngology. Oxford; Blackwell Science Ltd: 1997. 22.p. 161-164.
Brian P, Kelley BS, How to R, Samuel S. Evaluation and Reduction of Nasal Trauma. Journal of Plastic Surgery, Facial Trauma. 2010; 339-47. (accessed on May 22, 2015). Downloaded from: http://www.medscape.co.id.
Mendez DR, Lapointe A. Nasal Trauma and Fractures in Children. Available at. (accessed July 21, 2015). Retrieved from: http://www.uptodate.com
Anderson PJ. Fractures Of The Facial Skeleton In Children. J Otolaryngol Head and Neck. 1995; 26:47
Maniglia AJ, Kline SN. Maxillofacial Trauma In The Pediatric Age Group. Otolaryngol Clin North Am 1983; 16:717
Perkins SW, Dayan SH, Sklarew EC, et a. The Incidents Of Sports-Related Facial Trauma in Children. Ear Nose Throat J 2000; 79:632.
Gregory Staffel. Nasal Fracture. Current Therapy in Otolaryngology–Head and Neck Surgery. 6th ed. Saint Louis; Mosby Company: 1998. p.133-4
Chegar BE, Tatum SA. Nasal Fracture. In: Cumming CW, et all. Cumming Otolaryngology Head and Neck Surgery. 4 th ed. Baltimore; Mosby Inc: 2005. Chapter 41.
Stranc MF, Robertson GA. A Classification Of Injuries Of The Nasal Skeleton. Ann Plast Surg. 1979; 2.468
Weller MD, Drake AB. A Reviews of Nasal Trauma. Bri Med J. London 2006; 8
: 21-8. (accessed date 22 May 2015). Downloaded from http://www.amedeo.co.id
James KP, Robert MB. Nasal Fractures. In: Raymond JF, Robert VW, editors. Oral and Maxillofacial Trauma. Philadelphia: WB Saunders; 1991. p.600-15
Brian R, Bradley S. Management of Nasal Fractures. Arch Family Med. 2000; 9: 738-42. (accessed May 22, 2015). Downloaded from http://www.amedeo.co.id
Kucik CJ, et al. Management of Acute Nasal Fractures. In AAFP Journals. 2004; 70(7): 1315-20.(accessed date May 2 2015). Downloaded from http://www.BMJ.com
Smith JE, et al. Nasal Fracture Imaging. (Accessed July 19, 2015). Retrieved from http: //emedicine.medscape.com /article/ 391863-overviewl.
Daniel SY, Yea SH, Park HJ. A New Approach to the Treatment of Nasal Bone Fracture. Radiologic Classification of Nasal Bone Fracture and Its Clinical Application. J Oral Maxillofac Surgery. 2011; 69: 2841-47
Lalwani AK. Nasal Trauma. Current Diagnosis and Treatment Otolaryngology Head and Neck Surgery. Second ed. New York; Lange Mc Graw-Hill Company: 2007. Chapter 11.
Soetjipto D, Wardhani RS. Facial Trauma. In the Plastic and Reconstruction Study Group. Guideline for ENT-KL Diseases in Indonesia. Jakarta: 2003. p.82.
Kentjono WA. Management of Maxillofacial Trauma. PKB IX Health Sciences ENT-KL. Emergency Management in the Field of Ear, Nose, Throat-Head and Neck Surgery. Editor Ario Kentjono Widodo et al. Department/SMF Health Sciences ENT-KL FK UNAIR-RSUD Dr. Soetomo Surabaya: 2011. pp.165-181.
Corry JK, Timothy C, James P. Management of Acute Nasal Fractures. Am Fam Physics 2004; 70(7): 1315-20
Green KM, Board T, Mason JT. Alar Haematoma. J Laryngol & Otol 1999; 113: 1104-5. (accessed May 22, 2015). Downloaded from http://www.amedeo.co.id
Murphy J, Marshall AH, Jones NS. Restoration of the Impacted Nasal Pyramid Using Kirschner Wire. J Laringol & Otol 2004; 118: 543-5. (accessed 22 May 2015) Closed Reduction. Downloaded from http://www.amedeo.co.id
Richard LA, Robert H. Nasal Fracture. Cummings Otolaryngology Head and Neck. Chapter 42. 1990. p.1-17.Closed Reduction.
Wang FG, Kern EB. Nasal Fractures. In: Gates A. Current Therapy In Otolaryngology: Head And Neck Surgery. Philadelphia. PA; BC Decker: 1990: 105-109.Closed Reduction.
Kim JE, Park PH, Yoon CH. Analysis Of Nasal Septum Fracture Com- Bined In Nasal Bone Fracture Using Cr. J Korean Soc Plast Reconstr Surg 1998;25:852.Closed Reduction.
Rhee SC, Kim YK, Cha JH, et a. Septum Fracture In Simple Nasal Bone Fracture. Plast Reconstructive Surgery 2004;113:45-52.Closed Reduction.
Gerd JR, Carsten CB, Milo F, Jorg S. Technique and Timing for Closed Reduction of Isolated Nasal Fracture. A Retrospective Study. Ear Nose And Throat. J New York. 2002; 81(1):49-54.
Zargar M, Khaji A, Karbakhsh M, Zarei M. Epidemiology Study Of Facial Injuries During A 13 Month Of Trauma Registry In Tehran.Closed Reduction. Indian J Med Sci 2004; 58: 109-13
Comments