FOREIGN MASS IN RIGHT BRONCHUS IN CHILDREN
I Made Nudi Arthana
foreign mass in the bronchus is a object or material Good organic and inorganic which in a way physiological No There is in the tract tracheobronchial. Case object foreign tracheobronchial is Wrong One problem Which most occurs frequently in the world and is an emergency that can cause airway obstruction and be life-threatening.
LITERATURE REVIEW
Anatomy And Physiology Tracheobronchial Tract
The tracheobronchial tract is part of the lower respiratory tract that connects the larynx to the lungs, starting from the trachea and then continuing into the bronchi. bronchus And bronchioles. On Karina, trachea branching become 2 as high as T4 into the right and left main bronchi. Karina It is located further to the left of the median line, so that the lumen of the right main bronchus is wider than the left main bronchus. Bronchus main right more short from main bronchus left. Bronchus main right will branching become three, that is lobe right on, lobe right middle, And right lower lobe. The left main bronchus is divided into two, namely the left upper lobe and the right lower lobe. left below. 2.5 Size bronchus the more to lower will the more shrink and its structure even changed. Cell cilia or cell Which produce mucus No There are more on bronchioles so that particle foreign No Can issued through system mucociliary but will be phagocytized by macrophages in the alveoli. The ciliated columnar epithelium in the initial branching functions to warm and circulate air and to filter through the mucociliary role that pushes mucus upwards towards the esophagus. 6,7
Size tract tracheobronchial varies on person mature, man And women as well as in children and infants. The right main bronchus forms a 25 degree angle to the right. from line middle whereas bronchus main left make corner 45 degrees from line middle. With thus bronchus main right almost to form straight line with the trachea. 5 Other factors that facilitate the entry of foreign objects into the bronchus main right is Work muscle trachea Which push object foreign it is to the right. In addition, the inspired air into the right main bronchus is greater compared to the inspired air into the left bronchus. 2.7

Picture 2.1 Anatomy of the tracheobronchial tract
Table 1. Size tract tracheobronchial
Size | Man Mature | Woman Mature | Child | Baby |
Diameter trachea (mm) | 14 x 20 | 12 x 16 | 5 x 10 | 6 x 7 |
Long trachea (cm) | 12 | 10 | 6 | 4 |
Long bronchus right(cm) | 2.5 | 2.5 | 2 | 1.5 |
Long bronchus left (cm) | 5 | 5 | 3 | 2.5 |
Distance tooth on to trachea (cm) | 15 | 13 | 10 | 9 |
Distance tooth on to bronchus secondary (cm) | 32 | 28 | 19 | 15 |
Definition And Type Object Foreign Bronchus
Foreign body aspiration is the entry of objects from outside the body or from in body Which in condition normal No There is in channel breathing. Foreign objects in the respiratory tract are an emergency that requires immediate treatment. Delay in treatment can increase the occurrence of complications. even death. Aspiration object foreign in bronchus often causes respiratory disorders and is a cause of morbidity and mortality because it can cause acute respiratory disorders, chronic lung disease and even death. 1.2
Foreign bodies can be classified into exogenous foreign bodies (originating from outside the body) and endogenous foreign bodies (from within the body). Examples of endogenous foreign bodies are thick secretions (broncholiths), blood clots, crusts, pus, and meconium. While exogenous foreign bodies can be divided into solid foreign bodies (inorganic and organic), liquid foreign bodies (irritative and non-irritative), and gas. Inorganic materials are usually plastic, metal, toys and often fall into the asymptomatic phase and can be found incidentally. Organic foreign bodies such as grains, nuts, carrots, and corn tend to be more irritating to the mucosa and often cause more clinical symptoms. In addition, the shape of the foreign body also affects the clinical manifestations and extraction techniques, foreign bodies can shaped round, flat, irregular, And sharp. Object foreign Which enter into the respiratory tract can get stuck in the larynx, trachea, or bronchus, where 80 to 90% are found in the bronchus due to its size and configuration. 3,10
Epidemiology Object Bronchial Abnormalities
Statistical data mostly comes from single center studies . Several studies This estimate incident obstruction channel breath consequence object foreign is 0.66 per hundred thousand. According to data from the National Safety Council, tracheobronchial foreign bodies are one of the most common causes of unintentional death in children, where choking is the cause of 40% of deaths. children in lower age 3 year. Incident highest happen on child age 1 until 3 year And ratio man compared to Woman is 2:1 until
3:1.
In American Union, on year 2006 obtained as much as 4.100 case (1.4
per 100,000) child deaths caused by aspiration of foreign objects in the airway. Aspiration object foreign is reason number One death baby consequence accidents, and the fourth most common cause of death among preschool children younger than five years. Tracheobronchial foreign bodies have a unique demographic, 80% of cases occurring in children younger than three years, with a peak frequency occurring in the one- to two-year age group. In a series case retrospective as much as 81 case, Asif et al . report children under age five year Which experience aspiration object foreign as much as 77.8%, 16% by children aged between five And five twelve year, And 6.2% by children over fifteen years old. Likewise, Reilly et al ., highlighted that children aged four years or younger are more susceptible to foreign body aspiration due to exploration using a lack of a well-coordinated swallowing reflex. 1
In Indonesia, the Department of Broncho-esophagology, ENT, Faculty of Medicine, University of Indonesia, recorded 43 cases of aspiration that had undergone bronchoscopy from January 2002 to August 2004. In the Department of ENT-KL, Faculty of Medicine, Unand RS M. Jamil Padang recorded 8 cases of foreign body aspiration that had undergone bronchoscopy from January 2009 to March 2010. 3.7 Meanwhile, at RS dr. Muhammad Hoesin Palembang from January 2013 to March 2015, 19 cases of tracheobronchial foreign body aspiration were found, consisting of 2 cases in adults and 17 cases in children, of the 17 cases in children there was aspiration foreign objects made of metal in 6 cases. Foreign objects in the respiratory tract are more often found in the right bronchial system (52%). 1,3 Al-Sarraf, et al reported that the most common predilection for foreign objects stuck in the respiratory tract is the right main bronchus (32%) followed by the left main bronchus (23%), right lower lobe (17%), trachea (17%) and left lower lobe (11%). 5 Jaiswal, et al also reported that foreign objects in the respiratory tract are more often found in the right main bronchus (42-70%), followed by the left main bronchus (18.7-32.6%), trachea (27.5%), right segmental bronchus (22%), larynx (1-7.5%) and left segmental bronchus (3%). Object incident foreign tracheobronchial in General Hospital Sanglah Bali year 2012 until 2016
23 cases were found, where the most frequent location was in the right bronchus. namely 8 cases.
Etiology Object Foreign Bronchus
Object foreign on bronchus often happen on children consequence the tendency to eat while playing or running and cognitive abilities that are not yet fully developed so that it is difficult to distinguish which objects are edible and which are not. 1 The habit of putting objects in the mouth as a process of recognizing the environment which is a natural stage in its development. In addition, molar teeth in children have not fully grown so that it makes it difficult to chew food, coordination and control of the swallowing process are still Not yet Good, And there is immaturity in process elevation larynx and closing glottis. In older children, tracheobronchial foreign bodies are more often caused by anatomical abnormalities or neurological disorders. 3,11
There is a number of factor Which become reason object foreign enter to tracheobronchial tract, including: 3
a) Factor personal that is age, decline awareness, epilepsy And under the influence of alcohol
b) Factor physique: abnormality And disease neurological, process swallow Which not perfect in children, the nature and shape of foreign objects
c) Factor dental: medical And surgical (action extraction tooth, Not yet molar teeth erupt in children < 4 years old)
d) Factor mental health: disturbance emotion and psychic
e) Factor carelessness: put object besides food in mouth, meal preparation Which not enough Good, Eat in a hurry/while play, giving candy or nuts to children whose molar teeth have not yet fully grown
2.5 Pathophysiology Object Foreign Bronchus
Location stuck object foreign most often will stuck in 3 place, namely larynx, trachea, And bronchus. Proof literature show that incident foreign object in trachea seldom reported happen, that is only around 10–20% from all over
aspiration object foreign in road breath. Whereas, bronchus, especially bronchus right main, is the most common location for foreign body aspiration. The location where a foreign object gets stuck depends on the size, shape, and nature of the object. 2
Foreign object aspiration in children often occurs when children eat while screaming, laughing, or running with a foreign object in their mouth. food or object foreign can enter to channel breath on moment inspiration. On moment object foreign will pass plika vocalist , reflex closing plika The vocal cords will hold the foreign object so that it does not enter deeper, and with the help of the cough reflex the foreign object can come out. However, if the vocal cords defense is exceeded, the foreign object can be caught in the laryngeal sphincter which causes the patient to cough. paroxysmal (acute phase). In certain conditions, patients will not complain of significant symptoms (asymptomatic phase) which can occur for 24 hours. Respiratory symptoms and lung abnormalities can be seen depending on the nature and type of foreign object and the degree of obstruction caused by the foreign object. In general general, the more proximal stuck object foreign on the road breathing, the symptoms that arise will become more severe, rapid and obvious 3.6
Type blockage on bronchus according to Jackson (1936) is: 2.3
a. Bypass valve obstruction: blockage part from bronchus, often causes wheezing.
b. Ball valve obstruction: air inspiration And expiration Still Can in and out.
• Expiratory check valve obstruction (valve inhibitor expiration, obstruction like valve) : air inspiration can enter but difficult to get out, so it can cause obstructive pulmonary emphysema.
• Inspirational check valve obstruction (valve inhibitor inspiration)
: Inspiratory air is difficult to enter, but conversely, expiratory air is easy to exit, which can cause atelectasis.
c. Stop valve obstruction: inspired and expired air cannot enter/exit, which can cause atelectasis.
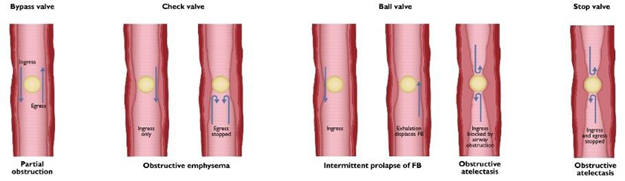
Picture 2.2 Type obstruction consequence object foreign. (A) Obstruction partial. Air can get out And enter, only cause wheezing. (B) Obstruction One direction. Air can enter However No can go out, cause emphysema lungs. (C) Obstruction total. Air cannot enter or exit, causing pulmonary atelectasis. 2
Complete obstruction of the main bronchus or intermediate bronchus can cause infection along the walk time, However on a number of case no symptoms are found if a foreign object is stuck in the main bronchus. Partial obstruction may cause local tissue inflammation with clinical signs of shortness of breath, wheezing, coughing, or other symptoms that vary depending on the airway structures involved. In general, the more proximally the foreign object is lodged in the airway, the more severe, rapid and obvious the symptoms will be. 1.5
Manifestation Clinical Object Bronchial Abnormalities
Part big object foreign on tract tracheobronchial No causing complete obstruction and clinical signs and symptoms vary depending on the size and location of the foreign body. 5 Clinical symptoms of foreign bodies in the tracheobronchial tract can be divided into three stages, namely the early period, the asymptomatic period, and the period with advanced symptoms/complications. 2
Period beginning (choking, gagging and wheezing)
These symptoms last for a short time. In this phase, the foreign object can be coughed out or become lodged deeper in the larynx and tracheobronchial tract .
Period without symptom (asymptomatic)
The respiratory mucosa can adapt to the presence of foreign objects and when matter the happen, so symptom beginning disappear. Period without Symptoms depend on the size and nature of the foreign body, and can happened for several O'clock or even a number of Sunday, And more often on object inorganic foreign. Most sufferer come look for help to hospital moment Already in This.
Period Complications
Symptom advanced due to by obstruction channel breath, inflammation, or trauma caused by foreign objects. The symptoms that arise vary depending on on location object foreign. On phase This, clinical Which found such as sputum mixed with blood, emphysema or atelectasis, the presence of fever due to toxemia, and other symptoms bronchiectasis, broncho-pneumonia and abscess lungs on chest x-ray.
The most common location for tracheobronchial foreign bodies to become lodged is in the bronchi. right. Object foreign tend enter to bronchus right by Because deviation angle bronchus right more small compared to left, diameter bronchus right bigger compared to left, air inspiration Which enter to bronchus right more much compared left, bronchus right almost parallel with trachea. Object foreign can totally obstruct the bronchus causing atelectasis, or cause check valve obstruction , which will then cause obstructive emphysema. Rupture of emphysematous bullae can occur spontaneously and result in pneumothorax. In addition, foreign bodies can move from one side to another, causing changes in clinical symptoms and signs. Foreign bodies that are left behind or remain can cause pneumonitis, bronchiectasis, or lung abscess. 3 Cases with foreign bodies in the respiratory tract Which reported as many as 120 (59.4%) cases that came from 0 to 48 hours after aspiration with complaint cough. As many as 70 (34.6%) cases with complaints of infection in the respiratory tract came 3 to 8 days after aspiration. It was found that 7 (3.5%) case with symptom bronchitis And pneumonia Which come on 9 up to 30 day after aspiration And the rest as much as 5 (2.5%) case with Symptoms of chronic bronchitis and bronchiectasis appear 1 to 8 months after aspiration. 7
Diagnosis Object Foreign Bronchus
Diagnosis of foreign bodies in the bronchus can be confirmed through anamnesis, inspection physique, And inspection support. Part most important when evaluating aspiration cases is the anamnesis given by the witness at the time incident. History choked I (cough repeatedly), wheezing, And stridor occurs in more than 90% of children who experience foreign body aspiration, and is often accompanied by transient perioral cyanosis. If the child has a fever, it is necessary to consider that the foreign body has been contaminated or is irritating and it is necessary to determine the time of the aspiration. the foreigner happen a number of Sunday even month Which Then, Which cause the child has pneumonia or a lung abscess.
On physical examination, clinical symptoms found include cough, tachypnea, decreased breath sounds, wheezing , stridor, dyspnea, cyanosis and suprasternal retraction. Decreased breath sounds occur in 30 - 60% of cases.
Initial supporting examinations that are often recommended in patients with foreign body aspiration in the tracheobronchial tract are radiological examinations. Radiological examinations have high information value for actions before endoscopy, examinations that are often It is recommended that a posterior anterior plain chest X-ray will show the location of the metal foreign body. (radiopaque) well. However, on object foreign Which radiolucent, like plastic, foreign objects are more difficult to see with just a plain X-ray examination. Abnormal images on radiological examination of patients with aspiration of foreign objects foreign is description like air trapped ( water trapping ), unilateral pulmonary hyperinflation, consolidation, collapse, atelectasis, tracheal shift and mediastinal shift, depending on the location and size of the foreign body.6,7,9 However , in some study previously, obtained around 50% case own results plain photo chest Which normal. On object foreign Which located in area larynx And trachea, examination of plain cervical anterior posterior and lateral radiographs can provide information. 8,9
Computed tomography (CT-Scan) of the chest can also be performed in certain cases when the results of a plain chest X-ray show normal results, but... complaint patient And history support suspicion to aspiration foreign objects. However, this method has high radiation exposure. In addition, cost factors and the availability of equipment and human resources must be considered. Fluoroscopy and MRI can be used as additional measures. Fluoroscopy examination is performed to view the entire respiratory tract. Examination the can evaluate moment inspiration And expiration And evaluate presence of mediastinal shift And widening intercostal (seen mediastinal shift to side lungs Which Healthy moment inspiration). Besides That can Also performed as guidance during the procedure ( C-arm ) if the foreign object is not visible during a regular bronchoscopy. Other examinations that can be performed are laboratory examinations to determine the presence of acid-base imbalance disorders and signs infection, can Also done inspection analysis gas blood And oxygen saturation level check. 1.9
Bronchoscopy is the first-line modality of choice for the diagnosis and management of bronchial foreign bodies. In preparation for bronchoscopy, other diagnostic tests may be performed to reduce complications and improve surgical success. 5 It should be noted that negative imaging findings do not definitively exclude a foreign body and endoscopy may be indicated if symptoms persist. 6
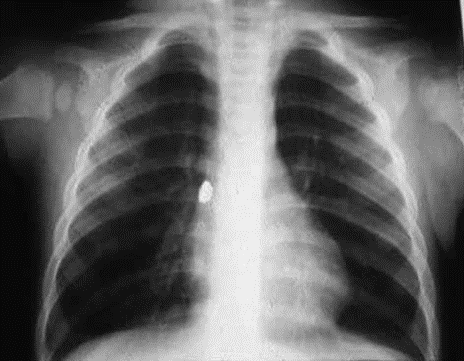
Picture 2.3 Description Photo plain chest aspiration object foreign (buffer earring) lodged in the first branch of the right bronchus
Treatment Object Foreign Bronchus
The principle of managing patients with foreign body aspiration is extraction. quick in a way endoscopic. Therapy supportive Which can given Before surgery is performed, oxygen is administered, steroids and preoperative antibiotics are administered, heart monitoring is performed, and oxygen saturation levels are checked.
Management of tracheobronchial foreign bodies depends on the location of the foreign body. If the foreign body is located in the trachea and bronchus, several actions are taken. operative Which can done is action bronchoscopy, cervicotomy, tracheostomy, and also thoracotomy. The actions taken depend on the type object And difficulty For do extraction. Extraction object foreign which actually has its own challenges. Edema, granulation tissue, and bleeding often hinder visualization in action extraction object foreign. In addition, edema in the airway after extraction is performed often results in airway obstruction. In this condition, intravenous corticosteroids and nebulized epinephrine are usually given. 7 Management chart on patient with suspicion object foreign located in bronchi can be seen in figure 2.4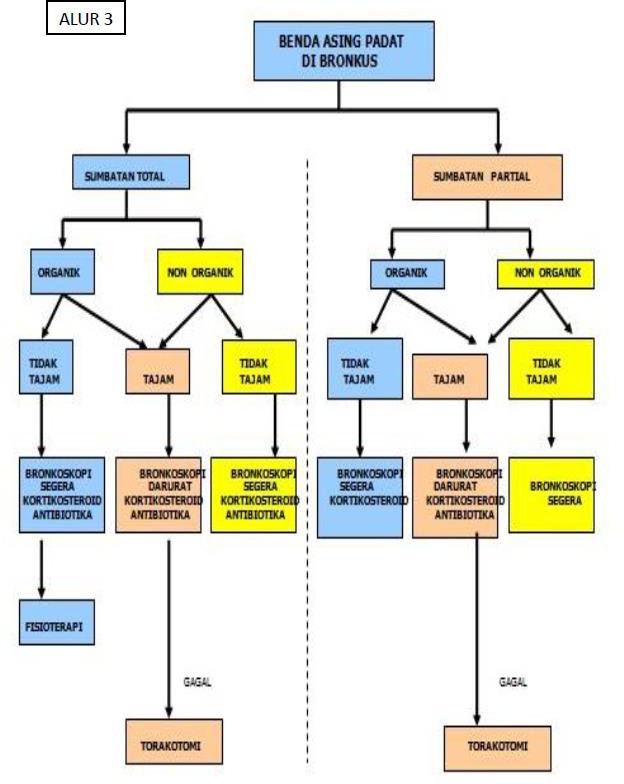

Picture 2.4 Charts governance object foreign in the bronchus. 3
Action operative Which often done is bronchoscopy. Bronchoscopy can be divided into two types, namely rigid and flexible bronchoscopy. Rigid bronchoscopy is more widely used to remove foreign objects from the bronchus. by Because can protect road breath moment extraction And Also with a larger lumen compared to flexible. Therapeutic approaches such as electrocauterization to control bleeding can be performed. 3
Flexible bronchoscopy allows better visualization of the distal airways and can be performed under local anesthesia and moderate sedation. Over time, with advances in bronchoscopic equipment and experience with flexible bronchoscopy, it has become the standard technique for the initial evaluation and management of aspirated objects. foreign to adults. While rigid bronchoscopy is the mainstay for foreign body removal in children and adolescents.

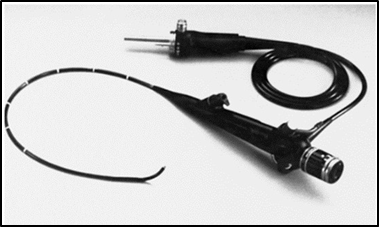
Picture 2.5 Rigid bronchoscopy And flexible bronchoscopy
Table 2 Comparison bronchoscope flexible And rigid
NO | Comparator | Bronchoscopy Flexible | Bronchoscopy rigid |
1 | Anesthesia | Topical AndGeneral | General |
2 | Track | Nose or via tracheostomy | Oral |
3 | Structure that is visible |
-Supraglottic
|
|
4 | Inspection in bed | Can done | No can done |
5 | Ventilation | Control ventilation hard to do | Control ventilation more Good |
6 | Removal of foreign objects | Difficult | Easy |
7 | Biopsy | Network Whichtaken just a little | Network Whichtaken more |
8 | Injury on the neck | Procedure candone | Procedure difficult done |
9 | Bleeding control | Difficult done | More easy |
Ng et al. compare bronchoscopy flexible and rigid including factors-factors to consider when choosing a modality in cases of aspiration of objects foreign mature. Found that bronchoscopy rigid more liked on patients without comorbidities, previous failed attempts at foreign body extraction, longer duration of aspiration and hard foreign bodies. Currently, rigid bronchoscopy is preferred because of its better ability to ventilate during surgery, better visualization, easier extraction of hard foreign bodies, greater flexibility because of the wider space provided to insert various sizes of suction and forceps so as to manipulate and facilitate the removal of foreign bodies from the airway. Rigid bronchoscopy is of 2 types, namely ventilating and venturi. 5 Bronchoscopy tools available in a number of size diameter and long. Selecting the right diameter is important because a size that is too large can cause edema in the trachea, the size of bronchoscopes in children can be seen in table 3.
Table 3. Recommendation Size Endoscopy Based on Child Age 5
Age | Size Bronchoscopy |
Neonate – 3 month | 3 |
4 – 24 months | 3.5 |
25 month – 3year | 3 ,7 |
3-6 years | 4 |
6-10 year | 5 |
> 10 years | 6 |
In do bronchoscopy extraction, needed instrument Which right for taking Which safe. Choice instrument depends on type, inorganic or organic, shape, size, and contour of the foreign body. Various types of forceps are available For used in extraction object foreign. Forceps varies depending on the presence or absence of teeth, the shape of the teeth (if any), the fenestration and the needle assembly placed in the center. Toothed forceps are used to hold objects Which No fragile like coin, bone And plastic. Forceps toothed Which The most commonly used are rat tooth, shark tooth and alligator forceps . Sharp objects or fine often clamped with forceps with the tip rubber for prevent injury on the surrounding airway tissue during extraction. Forceps are usually not used to remove fragile objects such as food and nuts. From results inspection radiology, size And location object foreign can be estimated, and become the basis for selecting the type of forceps. 4
Bronchoscopy has no absolute contraindications, but in certain conditions intervention with bronchoscopy is not recommended, namely in patients with airway difficulties such as neck that cannot be extended, spinal instability, kyphosis, trismus, and macroglossia. If severe edema occurs, repeat bronchoscopy is postponed for several days while waiting for the edema to subside using corticosteroids. In urgent situations such as asphyxia, bronchoscopy is postponed for 1-2 day until patient recover from shock, dehydration And fatigue. Besides That, The procedure should also be avoided in patients with weak physical conditions, severe hemoptysis, acute respiratory tract infections, aortic aneurysm, impaired heart and lung function, and have a risk of bleeding or blood clotting disorders. 3.5 If the patient has a tracheostomy, a flexible bronchoscope can be inserted through the tracheostomy stoma. 3.5
Postoperatively, if the patient requires observation, the patient should be treated in the intensive care unit, with adequate fluid monitoring to avoid dehydration. Clinical signs that must be monitored are mediastinitis such as fever, tachycardia, and tachypnea. Pediatric patients should remain intubated with observation in the intensive care unit. Sedatives should be given. avoided And suction periodic done For clean secret. When extraction object foreign done through tracheostomy, so can done suction secretions through a cannula with a small cannula size. 1,3,5
2.9. Complications Object Bronchial Abnormalities
Some complications that can occur in patients with foreign body aspiration and when foreign body extraction is performed are bleeding, asphyxia, and trauma. Bleeding can occur due to mucosal tissue injury during foreign body extraction. If the bleeding is not massive, it can be treated with electrocautery. CT angiogram pre-procedure can help evaluate risk of life-threatening bleeding during long-term foreign body extraction. A multidisciplinary approach is needed in foreign body extraction with difficult and sharp locations, namely by consulting the thoracic surgery department. 5
Asphyxia during action extraction object foreign is complications life-threatening. When large foreign bodies are extracted from the main bronchus, they sometimes become lodged in the trachea and can cause airway obstruction. Instrument manipulation can also cause and worsen laryngeal and subglottic edema, leading to airway obstruction. breath. 5 Accumulation Secret on bronchus often happen especially when foreign objects in the form of food, causing impending asphyxia due to the secretion itself.
Trauma on tape voice or laceration or perforation wall road breath may occur during extraction procedures. In cases of such complications, it is important to ensure adequate ventilation and control associated bleeding. 5
Foreign bodies can also migrate and the remaining foreign body fragments can block the distal bronchus. In children under 2 years of age with foreign bodies in the form of food, subglottic edema can occur which can be avoided by not performing repeated bronchoscopy. If subglottic edema occurs, a low tracheostomy, namely below the second tracheal ring, must be performed immediately. performed. 3 Surgical shock can occur in patients depending on the length of surgery. In infants, bronchoscopy is recommended for a maximum of 15 minutes, while for toddlers it is recommended for a maximum of 30 minutes.
If pneumonia is present, the patient may be given antibiotics. Corticosteroids such as intravenous dexamethasone (0.5 to 1.0 mg/kg) may be given to reduce postoperative edema. Bronchodilators may be given to help clear pulmonary secretions. 1.5 Depending on the difficulty of extraction, an X-ray may be performed 6 hours after surgery to detect complications of perforation and air in the mediastinum. Repeat X-rays are important, especially in children with compromised ventilation or oxygenation, which may be due to spontaneous pneumothorax, retained foreign bodies, or pneumonia. 1.3
REFERENCE
Rose D, Dubensky L. Airway Foreign Bodies. [Updated 2023, August 7]: Publishing StatPearls; 2023 January-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539756/
Dionysia Vidya Paramita, Sri Herawati June. Physiology And Function Mucociliary Bronchus. ENT Journal - KL Vol.9, No.2, May - August 2016, pp. 64 – 73
College of Otolaryngology, Head and Neck Surgery. Bronchoesophagology Module, 3rd Edition. 2022
Satish Chandra Tripuraneni, N. Priyadarshni, R. Venkataratnam, K. Rajanikanth, R. Naveen. Bilateral Foreign Body Bronchus . Indian Journal Otolaryngol Head Neck Surgery (October 2019) 71(Suppl 1): S400–S405; https://doi.org/10.1007/s12070-018-1325-4
Wackym P, Snow J. Ballenger's otorhinolaryngology head and neck surgery. 18th ed. 2016.
Dhingra, et a. Diseases of Ears, Nose and Throat & Head and Neck Surgery.
Divyansh Bajaj, Ashutosh Sachdeva, Desh Deepak. Foreign Body Aspiration. Journal of Thoracic Disease. 2021;13(8):5159-5175. http://dx.doi.org/10.21037/jtd.2020.03.94
Saw-Aung M, Kong RM, Cipriano N, et al. National Trends of Pediatric Aspirated/Ingested Foreign Bodies . Clin Pediatr (Phila) . 2023 Jun 28. 99228231181978.
Truong B, Luu K. Diagnostic clues for the identification of pediatric foreign body aspirations and consideration of novel imaging techniques . American Journal ofOtolaryngology. 2023 Jul;44(4):103919.
Bluestone, Charles D. Bluestone and Stool's Pediatric Otolaryngology 5th Edition, Volume 1(2014)
Bailey BJ, Ed. Head and Neck Surgeryotolaryngology . Vol.8. Philadelphia:JB Lippincott Company .h. 1782-91 Sixth Edition 2014
Lina Wang, Li Zhang, Deli Li, et al. Successful retrieval of plastic beads from the airway of child by flexible bronchoscopy and balloon-tipped catheter . Medicine 2018. 97:37
Ahmed, Abdul, Aziz, et al. Unusual method in tracheobronchial foreign body aspiration management.Clinical Suicide Research Communication 2020; 4(2)
Hesham, Alaa, Hemp. Management challenges in the passing through technique using a forgetful catheter to remove a endobronchial foreign body from an infant. The Ochsner Journal 2015. 15:110-113
Ravindra, Gaurab, Subhabrata et al. Successful removal of foreign body bronchus using C-arm guided insertion of forgetful catheter through plastic beads. Indian Journal of Critical Care medicine 2017. 21;36-38
Julie, Santhanam, John, et al. Marble in the right main stem bronchus: Management. Otolaryngology Head and Neck Surgery 2003; 128:287-9
Williams A, George C, Atul PS, et al. An audit of associated morbidity and mortality with foreign body aspiration in children from a tertiary level hospitals in Northern India. Afr J Paediatr Surg 2014;11:287–92.
Comments