FUNGAL RHINOSINUSITIS
I Made Nudi Arthana
Fungal rhinosinusitis is condition pathological on sine paranasal accompanied by inflammation sine Which caused by fungal infection. The etiology of fungal rhinosinusitis in Indonesia has not been widely documented. According to research conducted at the Haji Medan Hospital in 2014-2015, out of 74 cases of chronic rhinosinusitis that underwent fungal culture examination, there were 30 positive cases of fungi, most of which were found in the age range of 21-40 years, namely 60%. The distribution of fungi from the 30 cases that grew the most was Aspergilus fumigatus that is 15 sample (50%), Aspergillus sp as much as 7 sample (23.3%),
LITERATURE REVIEW
Anatomy of the Nose
The nose is pyramidal in shape and consists of a framework of bone and cartilage. Which covered by muscle And skin. Nose part outside consists of above the base nose ( bridge ), stem nose ( dorsum rice ), peak nose ( tips ), ala nasi, columella, and nostrils ( anterior nares ). Nasal bone framework consists of on: bone nose ( os nasal ), process frontalis OS maxilla and process nasal OS frontal. Whereas Cartilage located on two thirds The lower part of the nose consists of the superior lateral nasal cartilages, a pair of inferior nasal cartilages, the minor alar cartilages and the septal cartilages. 4 Parts nose in consists of on structure Which stretch from anterior nares until koana in posterior Which separate cavity nose from nasopharynx. The nasal septum divides the inner part of the nose into the nasal cavity right And left. Cavity nose consists of from part Which covered skin called the vestibule and the part lined by mucosa is called the nasal cavity. The vestibule is the anterior part of the nasal cavity. The vestibule is lined by skin. And containing gland sebaceous, follicle hair And hair – hair namely vibrissae. On part on vestibule that is on wall lateral there is style rice Which formed by cartilage nasal lateral superior. 4
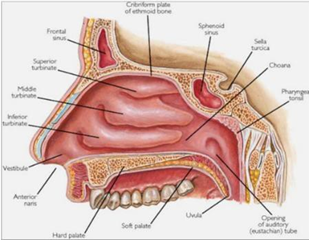
Picture 2.1 Anatomy Nose
Each cavity rice own 4 fruit wall, that is medial wall, lateral, inferior And superior. Wall medial nose is septum nasi formed by bone and cartilage. The septum is lined by perichondrium on the cartilage part and periosteum on the bone part, while the outside is lined by nasal mucosa. On the lateral wall there are 3 conchae, namely the inferior conchae which is the largest and located at the bottom, then the middle conchae, superior conchae. 4
Between the conchae and the lateral wall of the nose there are narrow cavities called meati, consisting of three, namely the inferior, middle and superior meatus. Meatus inferior located in between concha inferior to base nose and the lateral wall of the nasal cavity. In the inferior meatus there is the opening ( ostium ) of the nasolacrimal duct. The middle meatus is located between the middle concha and the lateral wall of the nasal cavity. In the middle meatus there are the openings of the frontal sinus, maxillary sinus and anterior ethmoid sinus. In the superior meatus which is the space between the superior concha and the middle concha there are the openings of the posterior ethmoid sinus and the sphenoid sinus. 4
The boundaries of the nasal cavity are in the inferior part where the floor of the nasal cavity is formed by the maxilla and palatine bones. In the superior part, the roof of the nose is very narrow and is formed by the cribriform plate that separates the cranial cavity from the nasal cavity. The cribriform plate is a plate of bone originating from the ethmoid bone. holes where the olfactory nerve fibers enter. In the posterior part, namely the roof of the nasal cavity which is formed by the sphenoid bone. 4
Anatomy Complex Ostiomeatal (COM)
The ostiomeatal complex (OMC) is a gap in the lateral wall of the nose that is bounded by the middle concha and the lamina papyracea. The important anatomical structures that form the OOM are the uncinate process, ethmoid infundibulum, semilunar hiatus, ethmoid bulla, agger nasi and frontal recess. The OOM is a functional unit that is the place of ventilation and drainage of the sinuses located anteriorly, namely the maxillary, anterior ethmoid and frontal sinuses. If there is obstruction in this narrow gap, there will be significant pathological changes in the related sinuses. 4

Picture 2.2 Complex Ostiomeatal
Anatomy Paranasal Sinuses
The paranasal sinuses are air cavities located in the head and are the result of pneumatization of the bones. There are four pairs of paranasal sinuses, starting from the largest, namely the maxillary sinus, the sinus frontal, ethmoid sinuses and sphenoid sinuses. All paranasal sinuses have openings (ostia) into the nasal cavity. 5
The paranasal sinuses are composed of ciliated mucosa and an overlying mucous membrane. In in the sinus, cilia move in a way regular For flow mucus towards its natural ostium follows certain patterned pathways. Mucus originating from the anterior sinus group that joins at the ethmoid infundibulum is drained into the nasopharynx in front of the eustachian tube opening, while mucus originating from the posterior sinus group joins at the sphenoethmoidal recess, drained into the nasopharynx postero-superior to the tube opening. This is why in sinusitis there is post-nasal secretion ( post nasal drip ), but there is not necessarily secretion in the nasal cavity. 5
The function of the paranasal sinuses is not yet known for certain, several theories have been put forward including regulating air conditions, maintaining temperature, helping with head balance, helping with voice resonance, dampening changes in air pressure and helping with mucus production. clean your nose. 5
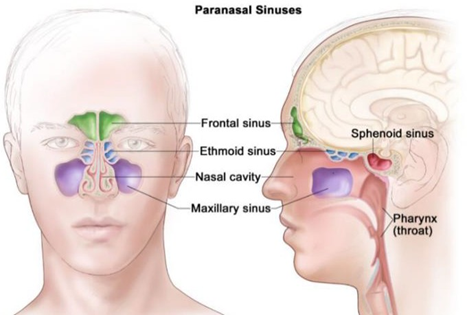
Picture 2.3 Anatomy Sine Paranasal

Picture 2.4 Charts estuary sine paranasalis
Histology
Consisting of above: 5
Pars vestibular : coated by stratified epithelium flat No keratinized
Pars respiratory: lined with ciliated stratified epithelium with goblet cells. In the lamina propria, there are many sero-mucosal glands that secrete to maintain the humidity of the incoming air, as well as superficial venous plexus to warm the air.
Olfactory pars: lined with stratified columnar epithelium. Consists of three cells, namely: sustentacular cells contain many microvilli, basal cells, and olfactory cells. In this area, there are also Bowman's glands (serous type).
The nasal and sinonasal mucosa consists of the epithelial layer, lamina propria, submucosa, and periosteum. The nasal mucosa and paranasal sinuses consist of stratified, ciliated, columnar epithelial cells. Between the epithelium are goblet cells. Goblet cells produce mucus.
Definition And Classification Rhinosinusitis
The Association of Ear, Nose, Throat, Head and Neck Surgeons (PERHATI-KL) defines rhinosinusitis as inflammation of the paranasal sinus mucosa and nasal cavity, rhinosinusitis is defined as inflammation of the nose and paranasal sinuses characterized by two or more symptoms, one of which includes nasal congestion or obstruction or congestion or discharge from the nose (anterior or posterior nasal drip) accompanied by facial pain and/or decreased sensitivity to smell, if it occurs ≤ 12 weeks it is said to be acute rhinosinusitis and if ≥ 12 weeks it is said to be chronic rhinosinusitis (CRS). 5,12 Based on its severity, it is divided into mild VAS 0-3, moderate VAS >3-7 and VAS weight >7-10 where VAS 0 is not disturbing and VAS 10 is very disturbing.
Based on its classification, rhinosinusitis is divided into primary and secondary. Primary CRS is divided based on its anatomy, local (unilateral) and diffuse (bilateral). Then it is divided based on endotype into type 2 and non-type 2 which is a division based on pathophysiological mechanisms, as well as based on its phenotype. Phenotype differentiated from symptom clinical, results nasoendoscopy, and CT-Scan. 6

Picture 2.5 Classification of Primary Chronic Rhinosinusitis

Picture 2.6 Classification Secondary Chronic Rhinosinusitis
Based on its duration, rhinosinusitis shared become :
Acute: sudden onset, duration <12 weeks and complete resolution <4 weeks
Rhinosinusitis I viral : duration <10 day
Post-viral acute rhinosinusitis: increasing symptoms > 5 days or duration > 10 days
Acute bacterial rhinosinusitis: colored mucus, severe local pain, fever > 38C, increased CRP levels, double sickening.
Chronic : longer duration from the same with 12 Sunday
Recurrence If There is ≥ 4 episode per year with intervals without symptom.
Based on post-therapy clinical assessment, rhinosinusitis is divided into controlled, partially controlled and uncontrolled. The controlled criteria are if no there is complaint And If even There is complaint No bother And mark VASE
>5 and on nasoendoscopy examination the mucosa appears healthy. At this stage no special management is required and only observation is needed for the next 6 months. Partially controlled assessment is if there is one significant complaint from all the symptoms felt by the patient and the VAS value is <5 and on nasoendoscopy examination there are signs of inflammation in the paranasal sinus nasal mucosa. At this stage the patient requires one stage of management so that there are no additional disturbing complaints. The uncontrolled criteria is if there are three or more disturbing complaints, with a value VASE >5 And on inspection nasoendoscopy obtained inflammation mucosa nose and paranasal sinuses. Maximal management (adequate surgery, intranasal corticosteroids and more than two short-term antibiotics or systemic corticosteroids in the last year) has been given. in this patient but did not reduce complaints or symptoms.
Definition of Rhinosinusitis Fungal
Fungal rhinosinusitis or rhinosinusitis caused by fungi is a disease that has a spectrum of clinical symptoms, histological features and biological abnormalities. Rhinosinusitis can occur acutely or chronically and is more often classified as invasive and non-invasive fungal rhinosinusitis which is categorized based on its tissue invasion. 1
Acute fungal rhinosinusitis is aggressive and has a clinical course of less than 30 days. Subacute rhinosinusitis has a clinical course of more than 90 days. However, currently, the classification used is invasive and non-invasive rhinosinusitis.
Classification
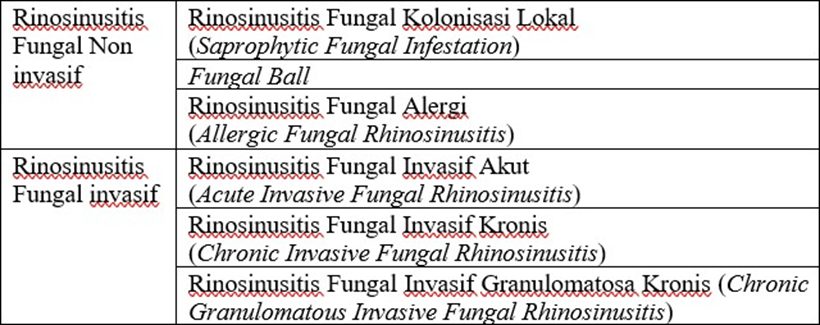
Fungal rhinosinusitis was originally classified based on the causative organism (such as aspergillosis or mucormycosis ). The shift from the causative organism to the pathology of the disease process occurred in 1965, when it was discovered that there were two broad categories, invasive or noninvasive, depending on the potential for fungal hyphae to invade tissue through the epithelium (invasive) versus infection confined to the superficial epithelium (noninvasive). As the name suggests, invasive fungal rhinosinusitis can result in extensive tissue invasion including mucosa, bone, neurovascular structures and adjacent organs. In addition to differences in pathology, there is some variability in the chronicity of the disease. 6
Table 2.1 Classification Rhinosinusitis Mold
Epidemiology
Fungal rhinosinusitis causes significant physical symptoms, significant reduction in quality of life, and can substantially interfere with daily functioning. The economic impact is also enormous, with direct costs estimated in the United States in 1996 at $5.6 billion per year, and indirect costs including >70 million lost activity days per year and reduced physical and social functioning. As the incidence of chronic rhinosinusitis has increased over the past decade, the economic impact is expected to be even worse. It should be noted that the prevalence of fungal rhinosinusitis is even greater in tropical countries such as India, Sudan, and Pakistan than in the United States. 1,7 In India, fungal etiology was found to be present in 30% of 100 people in the state of Tamil Nadu; 42.6% of 190 people in the JSS Hospital, Mysore, India; and 0.11% of 66,375 people spread across 42 villages in the states of Haryana and Punjab, India. 7,8,9
Data in Indonesia is not widely available regarding the cause of fungi in rhinosinusitis. A study at the Medan Haji Hospital in 2014-2015 from 74 cases of chronic rhinosinusitis that underwent fungal culture examination, found 30 positive cases of fungus, the most common found in the age range of 21-40 years, which is 60%. The distribution of fungi from the 30 cases that grew the most was Aspergilus fumigatus , which is 15 samples (50%), Aspergillus sp as much as 7 sample (23.3%), Aspergillus niger 4 sample (13.3%), Candida sp as many as 3 samples (10%) and the least is Aspergillus versicolor only 1 sample. 2 According to estimates made by Wahyuningsih et al. (2021) the prevalence of fungal rhinosinusitis in Indonesia is estimated at around 294,000 cases. 3
Etiology And Factor Risk of Rhinosinusitis Fungal
Although reason rhinosinusitis fungal has clear due to by Due to exposure to fungi from various species, there are several factors that contribute to the occurrence of fungal rhinosinusitis including geographic location, host factors, and causative agent factors.
Role Geographical Location
Geographical location may be an important determinant of the incidence of allergic fungal rhinosinusitis and invasive granulomatous fungal rhinosinusitis. Allergic fungal rhinosinusitis is found to be more common in India, North Africa, the Middle East, and parts of the United States such as the Mississippi Valley and the Southeastern and Southwestern United States. The warm and dry climates especially in northern India, Sudan, Saudi Arabia, and Arizona have recorded very high numbers of cases. Invasive granulomatous fungal rhinosinusitis is found exclusively in Sudan, India, Pakistan, and is rare in the United States. Fungal ball may also have some geographical limitations, as the maximum number of cases have been reported in France, Italy, and Taiwan. Approximately 30 cases of fungal ball per year are reported from Poitiers and Toulouse in France. Overall, 173 cases have been reported from a single center in Poitiers, France over a 14-year period (1989-2002). Italy is also endemic for fungal sinus ball disease . During an 11-year period (1994-2005), 81 cases were reported from a single center in Pavia, Italy. In Asia, fungal ball was reported in 126 cases in a hospital in Taiwan over an 8-year period (1995-2003). 1,7
Role Factor Host
Host factors are one of the determinants that need to be considered. Most forms of fungal rhinosinusitis are more common in men. Reasons Certain For trend This Not yet known. However, fungal ball more often found in middle-aged or elderly women. Acute invasive fungal rhinosinusitis is more common in older age groups, this is associated with risk factors such as diabetes and cancer chemotherapy that are common in this age group. In several studies from Sudan and northern India, allergic fungal rhinosinusitis was found to be more common in young adult males from rural areas than others. Based on the reports In this study, it was suggested that young adult males who regularly went to the field in hot, dry climates often suffered paranasal sinus mucosal injuries and acquired agents from the field. In some studies allergic fungal rhinosinusitis has been claimed to be associated with African-American race and poverty, although these findings are not conclusive. consistently demonstrated across studies. 1
Acute invasive (fulminant) fungal rhinosinusitis occurs mainly in people with disturbance system immune. Patient Which suffer disease Which associated with impaired neutrophil function, such as uncontrolled diabetes mellitus with or without ketoacidosis, hematologic and solid organ transplant malignancies, aplastic anemia, and hemochromatosis, or in patients undergoing iatrogenic immunosuppression with systemic corticosteroids or chemotherapeutic agents, are particularly susceptible to the development of this disease. An absolute neutrophil count of less than 500 cells/ml strongly correlates with the development of fungal rhinosinusitis. Inhalation mold such as Aspergillus and Zygomycetes is phenomenon which are harmless. However, in immunocompromised individuals, these fungi can break down the host defenses and spread in and along blood vessels and nerves, infecting sinonasal tissues and creating an acidotic environment of tissue necrosis that is ideal for fungal growth. Extensive use of steroids is also an important cause of the disease. Steroids work in two ways, namely by suppressing the normal inflammatory cell response and by inducing a diabetic stage . Other risk factors found to be associated with the development of acute invasive fungal rhinosinusitis include long-term antibiotic use, indwelling catheters , nasal intubation, metabolic abnormalities, prolonged hospitalization. For allergic fungal rhinosinusitis, a history of atopy determines condition. The existence of history atopy to mold Also has found in some cases of fungal ball . However, a history of previous sinus surgery is a more important risk factor for the occurrence of fungal ball . In a case-control study, endodontic treatment of the tooth was found to be a strong risk factor for the occurrence of fungal ball in the maxillary sinus. 1,7
Role Factor Agent
The agents causing different categories of fungal rhinosinusitis are described in Table 2.2. Zygomycetes are by far the most common cause of acute invasive fungal rhinosinusitis. The predominant zygomycete causing the disease is Rhizopus oryzae . The most common cause of acute invasive fungal rhinosinusitis in immunocompetent hosts in tropical areas, especially in India, is Apophysomyces elegans . The most common septate fungi causing acute invasive fungal rhinosinusitis in immunocompromised patients are Aspergillus fumigatus and Aspergillus flavus . In a review of the literature, 168 culture-positive cases were reported in the UK, 87% of which were due to dematiaceous fungi and 13% to Aspergillus spp. The most commonly implicated dematiaceous fungi were Alternaria alternata , Bipolaris spp. , Drechslera spp. , and Curvularia lunata . Interestingly in India, A. flavus was isolated in more than 80% of cases of allergic fungal rhinosinusitis, both in the southern and northern parts of the country. A. flavus was also isolated from 50% of patients diagnosed with allergic fungal rhinosinusitis in the Middle East. In granulomatous invasive fungal rhinosinusitis, A. Flavor is pathogen Which most general isolated. On the contrary,
A. fumigatus causes most cases of chronic invasive fungal rhinosinusitis. Biopsy samples collected from most cases with fungal balls appear sterile, although the fungus is detected on direct microscopy. Only 30-50% of these cultures show growth of the causative fungus, which is usually is Aspergillus fumigatus or Aspergillus Flavor and sometimes P. boydii . 1
Table 2.2 Mold reason various category fungal rhinosinusitis
Category Fungal Rhinosinusitis | Mold The Common Isolated |
Invasive fungal rhinosinusitis granulomatous | A. flavus |
Rhinosinusitis chronic invasive fungal | A. fumigatus, A. flavus (less common) |
Acute invasive fungal rhinosinusitis (fulminant/ necrotizing ) | Zygomycetes : Rhizopus oryzae Aspergillus fumigatus, Aspergillus flavus Apophysomyces elegans (especially in India) |
Colonization localized (sporadic infestation) | Aspergillus fumigatus, Aspergillus spp. other |
Fungal ball ( Mycetoma / Aspergilloma ) | Aspergillus fumigatus, Aspergillus fla vus, and sometimes P. boydii . |
Rhinosinusitis fungal allergy | Dematiaceous fungi in the United States, Alternaria alternata, Bipolaris spp., Drechslera spp., Curvularia lunata, Exserohilum, Aspergillus flavus in India and the Middle East |
Pathophysiology
The pathophysiology of fungal rhinosinusitis is still not fully understood, in order for the fungus to grow, the fungal hyphae and spores must penetrate the paranasal sinuses. This condition develops when there are several disorders in mucociliary clearance (MCC) and/or obstruction of the sinus ostium. A better understanding of the process is needed. that occurs in the epithelium, including specific and non-specific immunity, as well as understanding the physiological and pathological mechanisms of fungal rhinosinusitis so that therapeutic targets can be determined. 10
Several hypotheses of fungal rhinosinusitis are due to the host response to airborne fungal elements and the barrier hypothesis of immune system. The first hypothesis states that inhalation and fungal proteins are presented to sensitized T cells causing a cytokine response that activates eosinophils on the mucosal surface. The second hypothesis is that eosinophils target the fungus as an aberrant host defense response, with degranulation and tissue damage that cause rhinosinusitis symptoms. 12
Diagnosis And Symptom Clinical
The Association of Ear, Nose, Throat, Head and Neck Surgeons (2016) developed diagnostic criteria for the diagnosis of rhinosinusitis based on anamnesis and physical examination. However, supporting examinations can be performed to help establish the diagnosis. Available supporting examination modalities include computed tomography (CT) scan of the sinuses. paranasal and histopathological examination. 13
Rhinosinusitis Fungal Non Invasive
Rhinosinusitis Fungal Colonization Local ( Saprophytic Fungal Infestation )
Local colonization fungal rhinosinusitis is described as fungal colonization of sinonasal cavity secretions or crusted mucosa. This local fungal colonization usually occurs after surgical intervention that leaves the nasal mucosa inflamed or crusted, which is then infected with inhaled fungal spores. The most common type of fungus is Aspergillus . Local fungal rhinosinusitis colonization is not invasive and is limited to the crust or mucosa in the nasal cavity. Symptoms are usually asymptomatic, nasal odor, and the presence of dry crust flakes when blowing the nose. On nasal endoscopy examination, fungi are usually seen growing on the dry crust without being accompanied by invasion. 6
Fungal Ball
Fungal ball is defined as a dense collection of fungal hyphae located outside the mucosa ( extra-mucosally ), causing inflammation or minimal mucosal reaction. Previously, the term fungal ball was called 'Aspergilloma', because the most common fungus found is the Aspergillus species . Fungal balls often occur in only one sinus, and the most commonly affected is the maxillary sinus (94%) and the rest occurs in the sphenoid sinus. Unlike invasive fungal sinusitis, fungal ball usually occurs in immunocompetent patients and is reported to be more common in the elderly female population. The pathogenesis of fungal ball formation is not fully understood. As rhinosinusitis fungal colonization local, mechanism entry mold to sinus is through inhaled spores. As mentioned earlier, it is possible that previous surgery or mucosal injury may play a role. The occurrence of fungal ball rhinosinusitis is associated with a history of endodontic dental treatment, therefore a history of previous dental treatment (root canal treatment, implants) should be asked to the patient. The clinical symptoms that appear are usually symptoms due to mass effect, and symptoms of nasal obstruction, purulent rhinorrhea, post nasal drip, headache. From the nasal endoscopy examination, mild mucosal inflammation can be found. 6
Rhinosinusitis Fungal Allergy ( Allergic Fungal Rhinosinusitis )
Type third from fungal rhinosinusitis non invasive is Allergic fungal rhinosinusitis. This type is considered the most common form of fungal rhinosinusitis and has a presentation and series of findings similar to chronic rhinosinusitis. Several diagnostic criteria are used to differentiate allergic fungal rhinosinusitis from other forms of rhinosinusitis, namely through clinical, radiological, and histologic findings. Criteria The most widely used diagnostics are described by Bent and Kuhn (Table 2.3). However, there are a number of debate about evaluation system This, Because a number of matter which is described is not specific for allergic fungal rhinosinusitis. 6
Table 2.3 Criteria Bent And Kuhn (German) et al., 2019)
Criteria Major | Criteria Minor |
Type I Hypersensitivity (Immunoglobulin E assay, skin test or clinical history) | Unilateral Disease |
Nasal polyps | Asthma |
Radiological characteristics based on findings computed tomography | Erosion or expansion of bone in computed tomography |
The existence of eosinophilic mucinwithout invasion | Eosinophilia |
Coloring positive fungus | Crystal Charcot-Leyden onmucin |
Allergic fungal rhinosinusitis is usually seen in younger patients (21-33 years) who are not immunocompromised . It is thought to be more common in the general population. atopic. Symptom typical Which can found production mucus, calledeosinophilic mucin , which is a thick, dark-colored mucus secretion. This mucin typically contains eosinophilic inflammatory cells and Charcot-Leyden crystals . Symptoms are generally similar to chronic rhinosinusitis such as nasal congestion, hyposmia, post-nasal drip, facial tenderness and nasal polyps. 6
Rhinosinusitis Invasive Fungal
Rhinosinusitis Fungal Invasive I ( Acute Invasive Fungal Rhinosinusitis )
Acute invasive fungal rhinosinusitis can be defined as the presence of fungal hyphae in the sinonasal mucosa, submucosa, blood vessels or bone, within one month or less of rhinosinusitis symptoms, acute invasive rhinosinusitis is most often found in patients with immunocompromise , such as in patients with diabetes, impaired neutrophil function, human immunodeficiency virus (HIV) / acquired immunodeficiency syndrome (AIDS), hematological malignancies, and patients receiving chemotherapy. 6
Acute invasive fungal rhinosinusitis, although rare, is important because of its aggressive course and high mortality rate (approximately 50-80%). From the available literature, this does not appear to have changed significantly over the past 20 years. As the name suggests, acute invasive fungal rhinosinusitis different from form rhinosinusitis fungal non invasive, Because there is invasion especially to structure nerve And vascular (No only mucosa). Typically, fungal spores are inhaled, after which (due to disruption of the normal immunological response) the fungus grow on layer mucosa And attack structure neurovascular. This causes thrombosis with local to distant ischemia leading to necrosis. Necrosis will then cause spread beyond the infected sinus cavity to the surrounding tissue and bone. 6
There are two organisms that cause acute invasive rhinosinusitis, namely: common, which are usually from Aspergillus and Zygomycetes species . 6
In contrast to non-invasive forms of fungal rhinosinusitis, acute invasive rhinosinusitis is most commonly encountered in immunocompromised patients . Acute invasive rhinosinusitis is broadly divided into two categories and each own pathogen general Which related, like on patient diabetes (approximately 50%), especially if poorly controlled, and is often associated with diabetic ketoacidosis. In these patients, the most frequently isolated fungal species are the Zygomyecetes order . This is due to its affinity for acidic environments with high glucose concentrations. The second group is those who are immunosuppressed, such as patients with neutropenia, human immunodeficiency virus (HIV)/ acquired immunodeficiency syndrome (AIDS), hematological malignancies, and patients receiving chemotherapy. Although neutropenia is strongly associated with acute invasive rhinosinusitis, most This patient has hematologic malignancy. The species most frequently found in these patients is Aspergillus based on isolation results. Another condition associated with acute invasive rhinosinusitis is in patients with iron overload or renal failure and receiving deferoxamine for iron chelation. The mechanism associated is that some fungi (Rhizopus) can bind to deferoxamine . 6
Symptoms that often appear are fever (50%-90%), rhinorrhea, headache and facial pain, eye disorders such as diplopia. Supporting examinations must be carried out such as radiological examinations and biopsies to prove the presence of invasion. 6
Chronic Invasive Fungal Rhinosinusitis
Chronic invasive fungal rhinosinusitis is pathologically very similar to acute invasive fungal rhinosinusitis, but occurs via a much more chronic course (over months to years). This is partly because its occurrence more often on population immunocompetent. Because slower progression, the disease appears more hidden so that the usual symptoms are non-specific such as bloody nasal discharge, unilateral nasal obstruction, cacosmia , or as a mass in the nasal cavity or paranasal sinuses. can cause proptosis. Area other For invasion is through maxillary sinus, causing skin changes, or to the anterior cranial fossa, causing symptom neurological. Matter This Enough often misinterpreted as malignancy. Similar with rhinosinusitis fungal invasive I, Aspergillus And
Mucor is organism Which general found. 6
Chronic Granulomatous Invasive Fungal Rhinosinusitis
Chronic granulomatous invasive fungal rhinosinusitis is rarely seen in the western world. It is more common in North Africa, the Middle East, and Asia in either immunosuppressed or immunocompetent patients. Like acute invasive fungal rhinosinusitis and chronic invasive fungal rhinosinusitis, chronic granulomatous invasive fungal rhinosinusitis involves invasion beyond the submucosa. It is usually associated with Aspergillus species . The histologic difference is that the disease process forms noncaseating granulomas. The clinical symptoms that appear are proptosis with an enlarged mass in the nose, cheeks, and orbital involvement. Other symptoms are usually similar to chronic invasive rhinosinusitis. 6
Supporting investigation
Inspection Histopathological
Diagnosis of fungal infections of the nose and paranasal sinuses can generally be done directly or indirectly. Direct diagnosis aims to isolate and identify the fungus. Sampling is essential to accurately identify the fungus, by taking samples from the edge of the fungal lesion using sterile swabs . Then, it is important to send the sample in the appropriate temperature and appropriate media for the necessary examination (formalin-fixed and humidified Bouillon medium ). 13
Pathological examination is performed on tissue and mucus, to look for fungal agents, inflammatory cells, and the presence of specific reactions (eg Charcot-Leyden crystals). Staining can be done using: hematoxylin-eosin (HE), periodic acid-Schiff (PAS) or Gomori silver impregnation which can differentiate morphology more clear. Inspection histopathology Also is technique Which fast And relatively cheap. Inspection This allow to detect the presence of fungi and confirm tissue invasion 13
Discussion inspection pathology on part This focused on the characteristics of each type of fungal rhinosinusitis as follows:
Rhinosinusitis fungal non -invasive
Local colonization fungal rhinosinusitis ( Saprophytic Fungal Infestation ) Rhinosinusitis fungal colonization local is category Which made to explain colonization mold on channel sinonasal Which usually happened after procedure surgery or incident traumatic, Which results in inflammation and ulceration/crustation of the sinonasal mucosa in the presence of superficial fungal infection without tissue invasion. Although this form of fungal rhinosinusitis most A little explained in literature, form This can to precede fungal ball development .
Fungal Ball Histologically, fungal ball is characterized as an encapsulated fungal mass or a fungal mass embedded in a fibrinous necrotic exudate, with minimal mucosal inflammatory reaction (Figure 2.5). By definition, there is no tissue invasion or granulomatous reaction in the surrounding tissue. On microscopic examination, fungal ball can appear similar to allergic fungal rhinosinusitis, especially since both have a layered appearance. 14
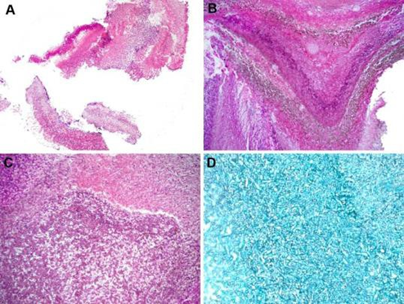
Picture 2.7 Description fungal histopathology ball . (A) low appearance power of fungal maxillary sinus ball . Fungal ball consists of an encapsulated mass of fungi (hematoxylin and eosin; original magnification ×10). (B) Low magnification fungal ball shows a layered appearance and fungi pigmented. Culture show Aspergillus niger (Hematoxylin And eosin; original enlargement
×25). (C) High magnification of fungal ball shows a mass of encapsulated fungus with minimal inflammation (hematoxylin and eosin; original magnification ×50). (D) Silver staining shows the presence of fungus in the fungal ball (Grocott stain; original magnification ×100) 6
Rhinosinusitis Fungal Allergy ( Allergic) Fungal Rhinosinusitis )
The main feature in patients with allergic fungal rhinosinusitis is the presence of clay-like mucin, brownish green or grayish in color. Microscopic examination shows eosinophilic mucin. which are mixed with detached epithelial cells, degranulated eosinophils, Charcot-Leyden crystals , and other inflammatory cells arranged in a laminar pattern and associated with scattered fungal hyphae (Figure 2.6 and Figure 2.7). Fungal hyphae are sometimes visible on hematoxylin and eosin stains, but are better seen with histochemical stains such as silver or PAS (Figure 2.6). 14
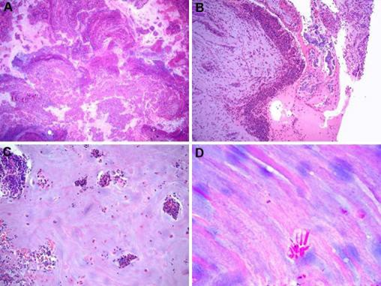
Figure 2.8 Histopathological features of allergic fungal rhinosinusitis. (A) Low-magnification view of allergic fungal rhinosinusitis showing a layered appearance with mucin. Which mixed with cell inflammation And debris (Hematoxylin And eosin; enlargement original ×10).
(B) Eosinophilic mucin shows clusters of eosinophils and detached epithelial cells (hematoxylin and eosin; original magnification ×50). (C) Eosinophilic mucin shows single and clustered eosinophils (hematoxylin and eosin; original magnification ×50). (D) Eosinophilic mucin shows Charcot-Leyden crystals (hematoxylin and eosin; original magnification ×200). 14

Figure 2.9 Histopathologic features of allergic fungal rhinosinusitis. (A) Eosinophilic mucin frequently contains bacterial colonies (hematoxylin and eosin; original magnification ×100). (B) Fungal organisms are rarely seen in eosinophilic mucin without the use of special stains. Cultures show Curvularia sp. (Hematoxylin And eosin; magnification original ×100). (C) Coloring silver stain of fungal organisms on eosinophilic mucin. Culture shows Alternaria alternata (Grocott stain; magnification original ×200). (D) Hybridization in there For Aspergillus ribosomal RNA in eosinophilic mucin. Culture confirmed A. fumigatus ( Nitroblue tetrazolium violet ; original magnification ×100). 14
Rhinosinusitis fungal invasive
Rhinosinusitis fungal invasive I
Histologically, the mucosa shows vascular thrombosis and inflammatory cells are usually few. When observed, it is common to see fungal angioinvasion forms resulting in lumen thrombosis. While fungi are usually seen on hematoxylin and eosin staining, silver and PAS staining are often useful to highlight the organisms especially in the vessel walls and lumen of the vascular space where they are often mixed with fibrin (Figure 2.8). Rapid diagnosis is essential because fungal forms can grow into vital structures including the orbit and cranial cavity, and patients with involvement of these structures have very high morbidity and mortality rates. 14
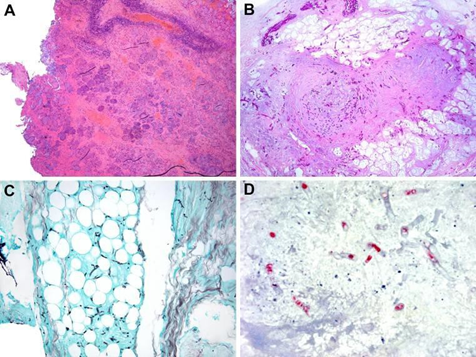
Figure 2.10 Histopathological features of acute invasive fungal rhinosinusitis. (A) Low magnification shows infarction without significant inflammatory reaction in an immunosuppressed patient with acute leukemia with acute invasive fungal rhinosinusitis. Culture shows Rhizopus sp. (Hematoxylin and eosin; original magnification ×12.5). (B) Acute invasive fungal rhinosinusitis shows fungus invading blood vessels and soft tissues. Culture shows Aspergillus fumigatus (Hematoxylin and eosin; original magnification ×100). (C) In Silver staining shows fungal hyphae in soft tissue in acute invasive fungal rhinosinusitis. Culture shows A. fumigatus (Hematoxylin and eosin; original magnification ×100). (D) In situ hybridization for Aspergillus ribosomal RNA shows extensive necrosis ( Fast red tetrazolium violet ; original magnification ×100) 14
The diagnosis of acute invasive fungal rhinosinusitis includes histopathological identification from form invasive mold to network, Which often done during intraoperative ( frozen section ). Frozen section provides immediate results so that it can planning is done care, which usually in the form of debridement followed by intravenous antifungal administration. Most cases are infected by either Aspergillus sp. or Rhizopus sp. . 14
Rhinosinusitis fungal chronic And chronic granulomatous
Chronic invasive fungal rhinosinusitis is a slow-growing invasive fungal infection characterized by invasion of numerous fungal organisms into the sinonasal mucosa with rare angioinvasion. This is in contrast to the chronic granulomatous type, which occurs in patients with immunodeficiency, organ transplantation, diabetes, and in patients treated with corticosteroids. A. fumigatus is the most common fungus found in cultures of these patients. In contrast to granulomatous fungal rhinosinusitis, more fungal organisms are found, inflammatory infiltrate is rare, and angioinvasion is sometimes present (Figure 2.9). The infection is characterized by submucosal granulomatous inflammation, rare fungal hyphae, and extensive fibrosis (Figure 2.10). The most common associated fungal organism is A. flavus.14
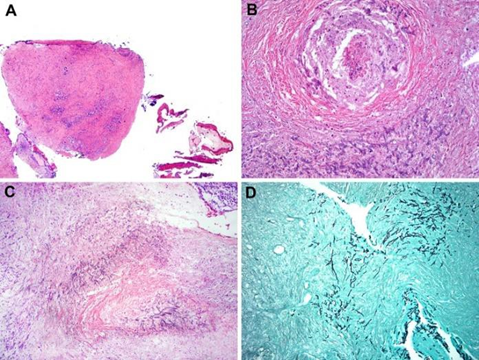
Figure 2.11 Histopathological features of chronic fungal rhinosinusitis. (A) Inflamed and fibrotic sinonasal mucosa in a liver transplant patient with chronic invasive fungal rhinosinusitis (hematoxylin and eosin; original magnification × 12.5). (B,C) Chronic invasive fungal rhinosinusitis with necrosis or infarction mucosa sinonasal Which wide with organism mold Which seen on liver transplant patient with symptoms for more than 3 months. (B) Fungi within blood vessels (Hematoxylin and eosin; original magnification ×100). (D) Silver stain shows fungal hyphae infiltrating the sinonasal mucosa (Hematoxylin and eosin; original magnification ×50). 14

Figure 2.12 Histopathological features of chronic granulomatous fungal rhinosinusitis. (A,B) Granulomatous reaction to Aspergillus flavus in a patient with chronic invasive granulomatous fungal rhinosinusitis (Hematoxylin and eosin; original magnification ×25 for A and ×100 for B). 14
Inspection Imaging ( Imaging )
Imaging plays a major role in the diagnosis of fungal sinus disease. Computed tomography scan without contrast remains the initial imaging study of choice in most cases. On the other hand, magnetic resonance imaging (MRI) is considered to better depict invasive conditions involving soft tissues outside the sinuses. Noninvasive fungal rhinosinusitis is characterized by sinus cover with high-density secretions on CT and T2 signal voids on MRI. 15
CT scan images is focused on each classification of fungal rhinosinusitis is as follows:
Rhinosinusitis fungal non -invasive
Rhinosinositis fungal colonization local ( Saprophytic Fungal Infestation )
No There is findings radiological special Which shown on this classification .
Fungal Ball
Fungal balls most commonly occur in the maxillary sinus (Figure 2.11). In addition, the sphenoid sinus is the next most commonly affected sinus. Sclerosis and thickening (referred to as osteitis) are the most common bony findings, followed by bony erosion and remodeling. Bony remodeling often results in enlargement of the sinus ostia (Figure 2.11). As classified, these lesions do not show evidence of tissue invasion. 15

Picture 2.13 Description CT Scan fungal ball . (A) Description piece axial without contrast And
(B) Coronal CT scan image shows a soft tissue mass with central calcification. The lesion extends into the left nasal cavity through the osteomeatal complex. The nasal septum is eroded and the fungal ball extends into the right nasal cavity. (C) Axial T2 magnetic resonance imaging shows a pseudopneumatized sinus. (D) Axial T1 image shows the sinus filled with material with higher intensity than the muscle. (E) Axial T1 postgadolinium fat-saturated image shows mucosal enhancement. (F) Endoscopic image shows the left nasal cavity with fungal debris protruding from the left maxillary sinus into the nasal cavity and eroding the nasal septum . MT, middle turbinate . 15
Rhinosinusitis fungal allergy ( Allergic Fungal Rhinosinusitis )
The diagnosis of allergic fungal rhinosinusitis relies on characteristic imaging findings. Bilateral and multisinus involvement is the most common characteristic, although unilateral multisinus involvement can also occur (Figure 2.12). 15
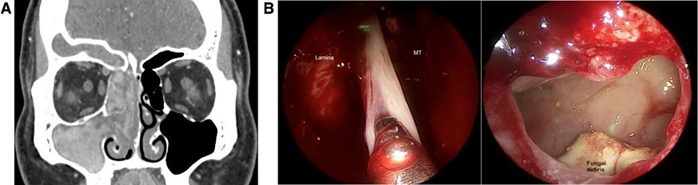
Figure 2.14 CT images of allergic fungal rhinosinusitis. (A) Coronal postcontrast soft tissue window computed tomography shows unilateral involvement of all sinuses on the right side. It appears to be diffuse within the right maxillary and frontal sinuses, and ethmoid. There is mild expansion of the ethmoid and frontal sinuses with bony remodeling. (B) Endoscopic image shows allergic or eosinophilic mucin originating from the right frontal sinus and also shows intraoperative endoscopic image of the right maxillary sinus after antrostomy showing fungal remnants. Lamina, lamina papyracea ; MT, middle turbinate . 15
Rhinosinusitis fungal invasive
Rhinosinusitis Invasive Fungal I
Unilateral thickening of the soft tissue mucosa of the nasal cavity is the most consistent early CT finding of acute fungal invasion. Severe thickening of the nasal mucosa along the conchae, nasal wall, and septum is seen in most cases. This radiologic finding is consistent with the endoscopic and surgical findings of significant mucosal edema and inflammation surrounding the area of ischemia (Figure 2.13 A and B). The findings are consistent with an early disease finding described on MRI called the black turbinate sign . The lack of contrast enhancement in the nasal cavity is due to mucosal necrosis that occurs in patients with mucormycosis , due to its angioinvasive nature. 15

Figure 2.15 CT images of acute invasive fungal rhinosinusitis. (A, B) CT scan without contrast shows submucous emphysema in (A) the right middle and inferior conchae and (B) the lateral nasal wall. (C) Endoscopic examination of the right nasal cavity, showing necrotic tissue in the right inferior conchae and the anterior part of the nasal septum. Endoscopic images of the nasal cavity right nose too shows extensive necrotic tissue to the concha media and inferior concha . 15
Bone erosion or extrasinus extension are both highly suggestive of acute invasive fungal rhinosinusitis, but are rarely seen in the early stages of the disease. Loss of periantral fat is a sign of invasion (Figure 2.13 C). When this is the only one findings radiological, infiltration network soft periantral may indicate the possibility of invasive fungal rhinosinusitis if the clinical picture in accordance (Picture 2.14 D). Expansion to intraorbital from ethmoid Also is features of acute invasive fungal rhinosinusitis (Figure 2.14 A and B). Periantral and intraorbital invasion may occur without evidence of bone erosion. 15
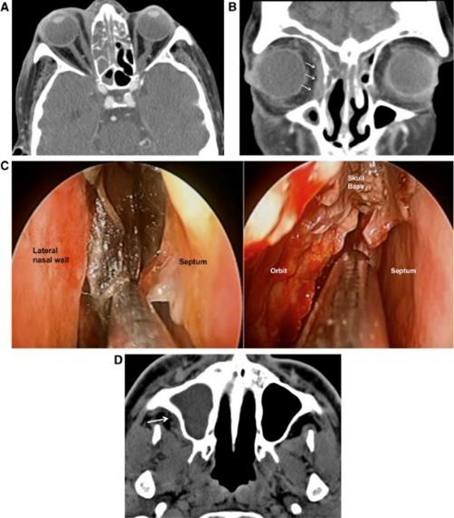
Figure 2.16 CT images of acute invasive fungal rhinosinusitis. (A) Axial and (B) coronal sections show soft tissue coverage in the right ethmoid air cell. Soft tissue extends into the medial periorbital fat, without erosion of the lamina papyracea . (C) Endoscopic examination beginning show network necrotic And formation crust congested fill in part upper right nasal cavity. Also shown is an endoscopic image showing necrotic tissue near the skull base and extending into the right orbit. The patient underwent debridement and exenteration of the right orbit. (D) Axial CT scan without contrast several days later shows periantral fat invasion through the posterior wall of the right maxillary sinus (arrow). 15
Rhinosinusitis Chronic Invasive Fungal
Chronic invasive fungal rhinosinusitis commonly occurs in the ethmoid and sphenoid sinuses. Because of the invasive nature of the disease, more involvement may be found outside the sinuses. Invasion most commonly occurs into the orbit (Figure 2.15 F). Intracranial invasion is the next most common location. A contrast-enhanced CT scan will show a homogeneously enhancing soft tissue mass (Figure 2.15 E). The affected sinuses are not significantly enlarged and bone erosion is localized to the site of extrasinus extension (Figure 2.15 B). 15
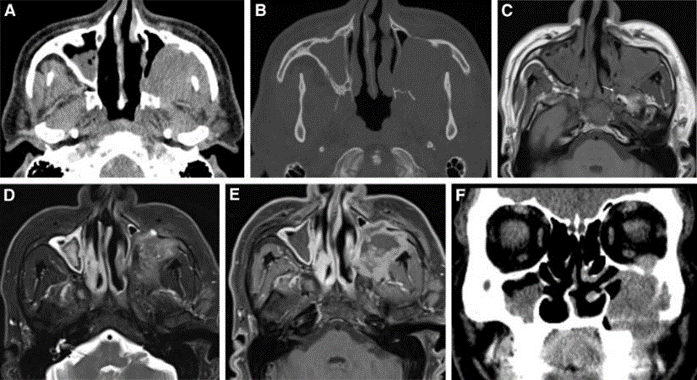
Figure 2.17 CT images of chronic invasive fungal rhinosinusitis. (A) Soft tissue window and (B) bone window computed tomography without contrast show a mass in the left maxillary sinus with lateral wall erosion. (C) Axial T1-weighted MRI without contrast shows extension into the pterygopalatine fossa (arrow). (D) T1 postgadolinium fat-saturated MRI shows a low-signal mass. (E) T1 postgadolinium fat-saturated MRI shows peripheral enhancement of the mass, with a nonenhancing central component . Resection shows granulomatous invasive fungal rhinosinusitis. chronic with network fibrotic congested, necrosis focal, And infiltrat inflammation chronic.
(F) Coronal CT scan without contrast shows erosion of the left inferior orbital wall with soft tissue extension into the orbit. 15
Rhinosinusitis Fungal Invasive Granulomatous Chronic
Imaging findings can be highly variable and it is not possible to differentiate chronic granulomatous invasive fungal rhinosinusitis from chronic invasive fungal rhinosinusitis by imaging alone. 15 The diagnosis is made by histopathology, in which the presence of noncaseating granulomas is characteristic. Fungal hyphae may be seen within Langerhans-type giant cells . This unique pathology distinguishes chronic granulomatous invasive fungal rhinosinusitis from chronic invasive fungal rhinosinusitis (Figure 2.16).

Figure 2.18 CT images of chronic granulomatous invasive fungal rhinosinusitis. (A) Bone window and (B) soft tissue window contrast enhanced computed tomography show a mass filling and extending into the left ethmoid sinus into the lamina papyracea . Proptosis is noted (left). (C) Axial T1 noncontrast MRI show mass isointense to muscle. (D) Axial T2 fat-saturated MRI shows a low-signal mass. (E) A xial T1 postgadolinium fat-saturated MRI shows a homogeneously enhancing mass. The imaging appearance is similar to chronic invasive fungal rhinosinusitis, but in this case the biopsy showed a poorly differentiated high-grade carcinoma 15
Inspection Other Support
The diagnostic method commonly used in patients with fungal rhinosinusitis is functional endoscopic sinus surgery followed by histopathological analysis. These samples are cultured and mixed with KOH for visualization under a microscope. 16
Mycological examination is also an important step in the analysis and can be performed with or without staining. Its sensitivity is comparable to histopathological examination. Sampling method, mucus is taken from the middle meatus or ethmoid, if there is suspicion of allergic fungal rhinosinusitis and examination is performed on days 2, 5, 7, 10 and 30. In other words, inadequate examination for a long period certain times can contribute to false negative results. 13
Serological examination aims to identify specific immunoglobulins that are markers of previous or current fungal infection. It should be noted that, in order to determine specific serum immunoglobulin G (IgG), two important conditions are required: the fungal antigen must have had sufficient contact with the with system immune host And system immune host must competent. Matter This explains why, in cases of local fungal rhinosinusitis infection (such as fungal ball ) in immunosuppressed patients (such as acquired immunodeficiency syndrome or leukemia), showing negative serology results. 13
Skin prick test is another very important diagnostic tool in the case of allergic fungal rhinosinusitis pathology. Recently, skin prick test has become the standard, and the fungal extracts used have been standardized for intradermal test. 13
Treatment Rhinosinusitis Fungal
To date, there is no internationally recognized guideline or consensus for the management of fungal rhinosinusitis. Surgical debridement is considered the treatment of choice for most cases of fungal rhinosinusitis, because it is both diagnostic and therapeutic. Functional endoscopic sinus surgery will allow the operator to observe the pathology and anatomy, perform biopsies of lesions, clean and wash the sinuses, and correct underlying problems (such as fistulas or foreign bodies). Polypectomy should be performed if indicated. 16
Oral corticosteroids are useful in many acute and chronic fungal rhinosinusitis and improve symptoms by suppressing inflammation and reducing circulating IgE levels, although long-term use is not recommended. Topical nasal steroids should not be used alone, but have a place in combination with systemic steroids. One study by Fokkens et al. showed benefit in reducing recurrence rates after two years. 16
Systemic antifungals are not ideal therapy for acute and chronic fungal rhinosinusitis, but may be an adjunct to invasive fungal rhinosinusitis. Amphotericin B may be the drug of first choice in the treatment of rhinosinusitis fungal invasive. Use a number of antifungal Azole class agents are also useful, but management with an infectious disease specialist is required. Topical antifungals have been reported with minimal efficacy, and are therefore not recommended. 16
Fungal immunotherapy is also an alternative treatment for acute and chronic rhinosinusitis, as it can reduce the body's sensitivity to fungal antibodies. Immunotherapy is an expensive treatment modality, and its short-term benefits outweigh its long-term benefits. However, immunotherapy can reduce the patient's need for corticosteroids and therefore prevent the side effects of long-term corticosteroid use. 16
Like mentioned on, part big rhinosinusitis cases fungal invasive is secondary to a compromised immune system. Therefore, the cause of immunodeficiency must be identified and addressed for optimal care . 16
Recommendations for management of fungal rhinosinusitis based on each classification are discussed as follows:
Rhinosinusitis Fungal Non- Invasive
Infestation Fungal Saprophytic ( Saprophytic Fungal Infestation )
The main relevance of this category of fungal rhinosinusitis is the speculation that it may be the starting point for the development of fungal ball . If symptomatic, it is usually treated with sinus surgery along with debridement. Nasal irrigation may be performed to moisten the mucosa. nose. Antifungal therapy is not used specifically in this condition, because the disease tends to recur, so repeat endoscopy is needed to monitor the results of treatment. 6,16
Fungal Ball
Since fungal ball is non-invasive, systemic or topical antifungal therapy is not recommended. The mainstay of fungal ball management is to improve the ventilation of the suspected infected sinus. Therefore, endoscopic widening or opening of the sinus ostium is necessary to restore normal sinus function. Surgical therapy, namely functional endoscopic sinus surgery (FESS) or if it is difficult to extract the fungal ball intact through the ostium, an external incision in the gingivobuccal ( Luc-Caldwell Operation ) can be an option. Management must be targeted on sine Which caught And factor the cause (that is fistula oroantral or dental amalgam residue). Fungal debris should be removed macroscopically and sinus lavage performed. It is also important to sample the surrounding mucosa, to rule out invasive fungal rhinosinus. 6
Rhinosinusitis Fungal Allergy ( Allergic) Fungal Rhinosinusitis )
Management of patients with allergic fungal rhinosinusitis may include medical and surgical interventions. However, patients often undergo several medical and surgical treatments before a diagnosis is made. According to Bent and Kuhn, allergic mucin and fungal debris are required to establish the diagnosis, which are most often found at the time of surgical intervention. 6
Good drainage and improvement of ventilatory function are the mainstays of therapy in patients with AFRS. Medical therapy with oral and topical steroids is recommended. The use of oral antifungals and immunotherapy is only used for refractory cases. Pharmacological therapies that are often used in AFRS are discussed as follows:
Therapy steroid
The widespread use of corticosteroids (oral and topical) has been shown to be beneficial in allergic fungal rhinosinusitis because they have been shown to suppress the inflammatory response, eosinophilia and IgE. There is reluctance to use prolonged oral therapy because of concerns about provoking adverse side effects. Evidence for the use of topical steroids alone is limited in allergic fungal rhinosinusitis. There is evidence to support their use in combination with oral steroids, resulting in a lower two-year recurrence rate (15%) when compared with placebo (50%). 6.10
Therapy antifungal
Oral antifungals have been used in the postoperative management of allergic fungal rhinosinusitis. Although allergic fungal rhinosinusitis is not a fungal infection, the goal is to reduce exposure to fungi and thereby reduce response immune due to mold. However, the benefits of oral antifungals are still debated. A Cochrane review of the efficacy of antifungal therapy on rhinosinusitis chronic with polyp nose fail show
any benefits. Meanwhile, according to Gan et al. concluded that The use of itraconazole type antifungals is beneficial in some patients and reduces the need for steroids. Given the side effects of systemic antifungals, oral antifungals are a last resort in patients who do not respond to steroid therapy. 6,10
Immunotherapy
Since the pathogenesis of allergic fungal rhinosinusitis is described as a type I hypersensitivity reaction, research has been developed to evaluate treatment with immunotherapy. Immunotherapy preparations in the form of subcutaneous immunotherapy, aim to limit the reaction to the exposed fungal antigen, just like immunotherapy For pollen in rhinosinusitis allergies. A systematic review of the literature found evidence ( grade C ) to support its use in allergic fungal rhinosinusitis. The evidence is somewhat limited, but there is a short-term (3-4 years) symptomatic benefit, although the long-term benefit is not well described. In addition to the symptomatic benefit, there is evidence to support its use in reducing the need for long-term postoperative steroid use. Given the limited evidence, long-term treatment and cost burden, immunotherapy may be a last resort for patients refractory to first-line treatment, as described above . 6,10
Modulator leukotrienes
The use of leukotriene modulators (such as Montelukast) has been reported from several literatures as AFRS therapy. One case study showed that Montelukast has benefits for AFRS refractory to conventional therapy. However, further studies are still needed to prove its efficacy. 6
Therapy biological
Recently, investigation of biologic therapies aimed at suppressing inflammatory mediators (e.g., anti-IgE and anti-IL-5 agents) has become a suggested treatment. These modalities have been extrapolated from their use in asthma. Early studies focused on the use of biologic therapies (for example omalizumab And mepolizumab) has show results Which promising. There was an increase in sinonasal outcome test (SNOT-22) scores (31%) and endoscopic scores (61%) in a population of patients with allergic fungal rhinosinusitis and asthma treated with omalizumab. 6,10
Rhinosinusitis Invasive Fungal
Rhinosinusitis Invasive Fungal I
The management of acute invasive fungal rhinosinusitis consists of three components: correction of predisposing conditions (i.e. neutropenia, ketoacidosis, etc.), debridement, and antifungal therapy. 6,10
Surgical intervention is an important element of therapy, through endoscopic sinus surgery early diagnosis can be made through tissue sampling. Another goal of surgical intervention is debridement of necrotic tissue (mucosa and bone if necessary). In this condition, debridement of necrotic tissue should be performed until healthy and bleeding tissue is found. This procedure may include removal of a large amount of nasal mucosa. large, conchae, as well as extended sinonasal access to clear the sinuses (e.g., medial maxillectomy, DRAF III, and others). In addition, quite often, repeated procedures are required to clear progressively developing necrotic tissue. 10
Early administration of systemic antifungal therapy has been shown to improve survival. To determine the right type of systemic antifungal, fungal culture results are needed. The antifungal drug of choice given is Amphotericin B at a dose of 0.25 mg/kg/day with a maximum dose of 1.5 mg/kg/day. However, early administration can cause side effects such as fever, nausea and hypotension and significant side effects have been reported, namely nephrotoxicity. If the culture results show Aspergillus , Voriconazole can be a therapeutic option. Voriconazole has a more minimal side effect profile, but is less effective in Mucorales . Other antifungals are available (such as Posaconazole, Isavuconazole), but both are used as second-line treatments and require a broader evidence base. Posaconazole is given to patients with kidney disease or patients at risk of kidney failure, namely in patients with uncontrolled diabetes. 6,10
Rhinosinusitis Chronic Invasive Fungal
Its implementation in a way general same with acute invasive fungal rhinosinusitis, with antifungal and surgical debridement. The principle of surgical resection is same, as is the approach to antifungal choice. 6
Rhinosinusitis Fungal Invasive Granulomatous Chronic
Management of chronic granulomatous invasive fungal rhinosinusitis is the same as other forms of debridement and systemic antifungals are the mainstay of therapy. 6,17
Complications Fungal Rhinosinusitis
In patients with immunocompromise, even though surgical therapy and systemic antifungal administration have been given, it can still cause several complications in the form of blindness, cerebral extension, cranial neuropathy , and death. In AFRS if therapy is not given adequately it can cause erosion of the surrounding bone, the presence of erosion is usually marked by symptoms of proptosis. In fungus ball, if not treated adequately it will cause worsening of rhinosinusitis symptoms and can invade the orbit to the central nervous system.
Rare but fatal complications are usually caused by invasive fungal rhinosinusitis, such as cavernous sinus aspergillosis or apical aspergillosis. orbita. When both the part caught, known as syndrome cavernous sinus-orbital apex. Patients may experience headache, acute unilateral loss of vision, or eye pain. This situation is usually caused by cavernous sinus thrombosis or carotid-cavernous fistula. 16
Tadros et al. (2022) in their study involving 45 patients with orbital complications in acute invasive fungal rhinosinusitis, reported that 18 patients had preseptal cellulitis, 13 patients had orbital cellulitis, and 10 patients had orbital apex syndrome. In total, four people were diagnosed with cavernous sinus thrombosis. Most patients (95.55%) had the condition immunocompromised consequence diabetes mellitus. Ophthalmoplegia And painful orbital is the most common ocular manifestation, followed by proptosis and relative afferent pupillary defect. The overall survival rate of patients was 66.67%. 17,18
In addition to complications due to the natural course of the disease, intraoperative and postoperative complications have also been reported in the study of Chaurpagar et al. (2023) involving 146 patients with acute invasive fungal rhinosinusitis. Similar to the study of Tadros et al. (2022), Chaurpagar et al. also found diabetes mellitus as the most common comorbidity and cause of immunocompromise in patients. Intraoperative complications recorded included bleeding (72.60%), cerebrospinal fluid leak (4.1%), orbital hematoma (0.68%), nasolacrimal duct trauma (2.05%), periorbital hematoma (0.68%). Postoperative complications reported included synechiae (56.16%), oroantral fistula (45.89%), hypoesthesia (25.34%), decreased visual acuity (16.43%), painful face (20.54%), abnormality form face (20.54%), diplopia (6.8%), Sick head (30.13%), anosmia (39.72%), Sick tooth (20.54%), Sick ear (9.58%), hyposmia (45.89%), ecchymosis periorbital (0.68%), residue disease (16.10%), relapse (2.05%), even death (2.05%). 17.18
Prognosis Rhinosinusitis Fungal
The prognosis in patients with allergic fungal rhinosinusitis is usually good. Allergic fungal rhinosinusitis is usually responsive to surgical treatment, and recurrences can be controlled. In contrast, invasive fungal rhinosinusitis is potentially life-threatening and has a poor prognosis. Invasion causes complications such as cavernous sinus thrombosis and central nervous system infection with a mortality rate of about 50%, so immediate treatment is needed. Complications can occur rapidly, and disease recurrence is high, and repeated debridement is often required. Some patients who recover may experience facial deformities, nerve damage, and chronic pain. The main prognostic factor is the patient's immune status. If immunity can be restored, the prognosis can be better. If the immune status cannot be restored, the prognosis is poor. 16
REFERENCE
Chatterjee, S.S., & Chakrabarti, A. (2009). Epidemiology and Medical Mycology of Fungal Rhinosinusitis. An International Journal of Otorhinolaryngology Clinics . https://doi.org/10.5005/jp-journals-10003- 1001
Harahap, NIK, Siregar, SM, & Nasution, MES (2018). Germ Profile in Nasal Secretions of Chronic Rhinosinusitis Patients at Home Medan Hajj Hospital. Ibn Sina Biomedical Journal , 2 (1).
Wahyuningsih, R., Adawiyah, R., Sjam, R., Prihartono, J., Ayu Tri Wulandari, E., Rozaliyani, A., Ronny, R., Imran, D., Tugiran, M., Siagian,
FE, & Denning, DW (2021). Serious fungal disease incidence and prevalence in Indonesia. Mycoses , 64 (10), 1203–1212. https://doi.org/10.1111/myc.13304
Soetjipto D, 4 E, Wardani RS. Nose. In Soepardi EA, et al. Textbook of Ear, Nose, Throat, Head & Neck Health Sciences. 7th Edition. Faculty of Medicine, University of Indonesia. 2012; pp.118-122.
Soetjipto D, E. Paranasal Sinus. In Soepardi EA, et al. Textbook of Ear, Nose, Throat, Head & Neck Health Sciences. 7th Edition. Faculty of Medicine, University of Indonesia. 2012; pp.145-149.
Deutsch, P. G., Whittaker, J., & Prasad, S. (2019). Invasive and Non-Invasive Fungal Rhinosinusitis—A Review and Update of the Evidence. Medicina , 55 (7), 319. https://doi.org/10.3390/medicina55070319
Chakrabarti, A., Rudramurthy, S. M., Panda, N., Das, A., & Singh, A. (2015). Epidemiology of chronic fungal rhinosinusitis in rural India. Mycoses , 58 (5), 294–302. https://doi.org/10.1111/myc.12314
Suresh, S., Arumugam, D., Zacharias, G., Palaninathan, S., Vishwanathan, R., & Venkatraman, V. (2016). Prevalence and Clinical Profile of Fungal Rhinosinusitis. Allergy & Rhinology , 7 (2), ar.2016.7.0156. https://doi.org/10.2500/ar.2016.7.0156
Shetty, S., Chandrashekar, S., & Aggarwal, N. (2020). A Study on the Prevalence and Clinical Features of Fungal Sinusitis in Chronic Rhinosinusitis. Indian Journal of Otolaryngology and Head & Neck Surgery , 72 (1), 117–122. https://doi.org/10.1007/s12070-019-01769-w
Lucia, C., & Alexandru, S. (2018). Fungal rhinosinusitis: pathophysiology, diagnosis and treatment. The Moldovan Medical Journal , 61 (2). https://doi.org/10.5281/zenodo.1299033
Bhushan B, Homma T, Norton JE, et al. Suppression of epithelial STAT1 activation by extracts of Aspergillus fumigatus. Am J Respir Cell Mol Biol. 2014
Association of Ear, Nose, Throat, Head and Neck Surgery Specialists. (2016). Sinusitis Chronicle. In Guide Practice Clinical in Ear Nose Throat-Head Neck Field Volume 1 (pp. 4–6). http://perhati-kl.or.id/wp-content/uploads/2017/05/ppk-perhati-vol1- okt2015.pdf
Patrascu, E., Manea, C., & Sarafoleanu, C. (2016). Difficulties in the diagnosis of fungal rhinosinusitis – Literature review. Romanian Journal of Rhinology , 6 (21), 11–17. https://doi.org/10.1515/rjr-2016-0001
Montone, K. T. (2016). Pathology of Fungal Rhinosinusitis: A Review. Head and Neck Pathology , 10 (1), 40–46. https://doi.org/10.1007/s12105-016-0690-0
This Mhurchu, E., Ospina, J., Thank you, A. S., Shewchuk, J. R., & Vertinsky,
AT (2017). Fungal Rhinosinusitis: A Radiological Review with Intraoperative Correlation. Canadian Association of Radiologists Journal , 68 (2), 178–186. https://doi.org/10.1016/j.carj.2016.12.009
Akhondi, H., Woldemariam, B., & Rajasurya, V. (2022). Fungal Sinusitis . StatPearlsPublishing.https: //www.ncbi.nlm.nih.gov/books/NBK551496/#:
~:text=Fungal sinusitis is a rare, also occur in immunocompetent patients.
Chaurpagar, R., Chiplunkar, B., Doifode, P., & Athawale, N. (2023). Study of Clinicoepidemiology and Surgical Complications in Acute Invasive Fungal Rhinosinusitis. Indian Journal of Otolaryngology and Head & Neck Surgery . https://doi.org/10.1007/s12070-022-03430-5
Tadros, D., Tomoum, M. O., & Shafik, H. M. (2022). Orbital Complications of Acute Invasive Fungal Rhinosinusitis: A New Challenge in the COVID-19 Convalescent Patients. Clinical Ophthalmology , Volume 16 , 4011–4019. https://doi.org/10.2147/OPTH.S391188
Comments