Kartagener's Syndrome
I Made Nudi Arthana
Kartagener's Syndrome (KS) is disease genetics recessive autosomal which accounts for about 50% of primary ciliary dyskinesia (PCD) cases. Because it is accompanied by various complications, PCD/KS greatly affects the quality patient's life. Syndrome This rare And First time described by Siewert on in 1904; however, Kartagener recognized the clinical syndrome in 1933. This syndrome includes the clinical triad of chronic sinusitis, bronchiectasis, and situs inversus. Camner et al. first suggested ciliary dyskinesia as the cause of this syndrome in 1975. In 1977, Eliasson et al. first coined the term "immotile cilia syndrome" to categorize infertility with chronic sinopulmonary infection. 1,2
LITERATURE REVIEW
Definition And Epidemiology
Siewert first described the combination of situs inversus, chronic sinusitis, and bronchiectasis in 1904. Manes Kartagener first recognized this clinical triad as a distinct congenital syndrome in 1933. Because Kartagener described this syndrome in detail, it was named taken from his name. Kartagener's Syndrome (KS) inherited through an autosomal recessive pattern. The symptoms are caused by defective ciliary motility. 2,3
Recurrent otitis media is a common manifestation of primary ciliary dyskinesia. Examination may reveal a retracted tympanic membrane with poor or absent mobility and middle ear effusion. Further testing usually shows a flat tympanogram and bilateral conductive hearing loss due to thick middle ear effusion. Many patients undergo repeated tympanostomy tube placement, often complicated by chronic suppurative otitis media. Otologic disorders associated with primary ciliary dyskinesia include tympanosclerosis, cholesteatoma, and keratosis obturans. 1
The incidence of Kartagener's syndrome is 1 case per 10,000-20,000 live births. Situs inversus occurs randomly in half of patients with primary ciliary dyskinesia; therefore, for every patient with Kartagener's syndrome, there is one other patient with primary ciliary dyskinesia but no situs inversus. inversus. Clinical manifestations sinusitis chronic, bronchitis, and bronchiectasis more critical during decade First life, but on Some cases improve in late adolescence.3,4
Etiology
The cause of primary ciliary dyskinesia is genetic, with an autosomal recessive inheritance pattern. Genomic analysis has found that primary ciliary dyskinesia is genetically heterogeneous. The DNAH5 and DNA11 genes at band 5p15.1 and 9p13,3, known causes dyskinesia primary ciliary. Second gene that encodes dynein. However, there are more than 200 genes thought to be involved. in biology cilia And Possible play a role in dyskinesia ciliary primary and other ciliopathies.5,6
Recently, a gene protein, CCDC40, has been characterized as a protein Which play role important on syndrome This. Mutation on protein This results in cilia with a reduced motility range and likely results in a variant of primary ciliary dyskinesia characterized by mislocalization of the central pair of microtubules and defective assembly of the inner dynein arm and dynein regulatory complex. 5,6
Loss-of-function mutations in CCDC114 cause primary ciliary dyskinesia with lateral malformations. The result of this mutation is loss of the outer dnein arm. Fertility does not appear to be significantly affected by the deficiency. CCDC114. Adenylate kinase type 7 (AK7), mediator reaction ADP to ATP and AMP, was also significantly reduced in patients with primary ciliary dyskinesia compared to healthy controls. AK7 expression also correlated with ciliary beat frequency in this patient population. 3.5
Pathogenesis
Camner and colleagues first suggested ciliary dyskinesia as a cause of Kartagener's syndrome in 1975. They described two patients with Kartagener's syndrome who had immotile cilia and immotile spermatozoa. These patients had poor mucociliary clearance because the cilia lining the upper airways were nonfunctional. 6,7
Later, Afzelius found that bronchial mucosal biopsy specimens from patients with similar respiratory complaints showed abnormal-looking, less motile cilia. In 1977, Eliasson and colleagues used the descriptive phrase "immotile cilia syndrome" to characterize male patients with infertility and chronic respiratory infections. 7
On year 1981, Rossman And his colleague create term primary ciliary dyskinesia (PCD) because some patients with . Current nomenclature classifies all congenital ciliary disorders as primary ciliary dyskinesias to distinguish them from acquired types. Kartagener's syndrome is part from group abnormality Which more big Which called as primary ciliary dyskinesia. Approximately half of patients with primary ciliary dyskinesia have situs inversus and, thus, are classified as having syndrome Kartagener. Afzelius proposed that the normal ciliary pulse required For rotation visceral during development embryo. On patients with dyskinesia ciliary primary, rotation organ happen in a way random; by Because That is, half of the patients had situs inversus and the other half had situs normal. 7,8
Ciliated epithelium covers most of the upper respiratory tract, including the nasal mucosa, paranasal sinuses, middle ear, eustachian tube, and pharynx. The lower respiratory tract contains ciliated epithelium from the trachea to the respiratory bronchioles. Each ciliated cell produces about 200 cilia that vary in length from 5-6 μm and taper to 1-3 μm as the airway narrows. 7,8
The typical ciliary axoneme consists of two central microtubules surrounded by 9 microtubular doublets. Each doublet has an A subunit and an A subunit. B Which attached as half circle. Sheath center envelops the two central microtubules, which attach to the outer doublet with radial spokes . 7, 8
The outer doublets are interconnected by nexin linkages, and each A subunit is attached to two dynein arms containing adenosine triphosphatase; one inner and one outer arm. The main function of the central sheath, the spokes radial, And link nexin is For guard integrity structural ciliary, while the dynein arm is responsible for ciliary movement. 7,8
The cilium is anchored at its base by cytoplasmic microtubules and a basal body consisting of a basal foot and a rootlet . The orientation of the basal foot determines the effective direction of ciliary movement. Just above the base, the cilium consists of a triplet of microtubular (previously doublet) without structure Which related, but in At the end, only the B subunit remains. 7,8
The cilia propel mucus over them through a two-part ciliary beat cycle. First, pulse power happen when cilia Which fully elongated move perpendicular to the cell surface in a curved manner. Then, followed by with pulse recovery, in where all over cilia bend And return to starting point near the cell surface. Once the cilium starts moving, a complete beat cycle is required. 7,8
Cycle this is mediated by dynein arm of subunit A Which attach to the subunit B from microtubules Which close together. Adenosine triphosphate hydrolyzed by dynein arms and 9 microtubule doublets as they rub against each other . 7,8
Patient with dyskinesia ciliary primary show various type defects in ciliary ultrastructure and motility, which ultimately impair ciliary beats and mucociliary clearance. The most common defect, first described by Afzelius, is a reduction in the number of dynein arms, which decreases ciliary beat frequency. 6,7
Other ciliary defects include abnormal basal cell apparatus with giant roots and double feet , cilia lacking all internal microtubular structures, and even cilia twice the normal length that beat in an uncoordinated, undulating manner. Some patients with the clinical picture of primary ciliary dyskinesia have normal-appearing ciliary ultrastructure, but irregular arrangement and direction of beats, leading to inefficient mucociliary transport. These findings illustrate the importance of analyzing ciliary motility and ultrastructure when considering the diagnosis of primary ciliary dyskinesia. Ciliary dyskinesia network primary Also marked with disturbance current transport ion chloride. Current This disruption has been shown to persist even after application of cAMP- enhancing agonists.6,7,8
Diagnosis
Diagnosis enforced based on anamnesis, inspection physique And supporting examination. 1.3
Anamnesis
In general, from the anamnesis, patients come with chronic upper and lower respiratory tract infections caused by ineffective mucociliary mechanisms. Patients come initially in the neonatal period, showing ineffective ciliary movements that are needed to clear the airways. fluid lungs fetus. As many as 80% baby Which new born with Primary ciliary dyskinesia is characterized by respiratory distress in the first 12-24 hours of life. The patient also complained of chronic productive cough with unexplained respiratory distress. This cough was described as wet and productive, found in almost 100% of infants. Coupled with unexplained drainage. appropriate on system sinonasal, matter This cause nose clogged, rhinorrhea, and chronic middle ear effusion with possible purulent otorrhea.
Some male patients present later in life with infertility due to immotile spermatozoa. Women may have a higher rate of ectopic pregnancy. more tall. Final, abnormality site reverse on imaging relatively specific for Kartagener's syndrome.
Physical examination
Primary ciliary dyskinesia is characterized by the clinical triad of chronic sinusitis, bronchiectasis, and situs inversus. The majority of patients are seen by physicians more than 50 times before the diagnosis is made at an average age of 10-14 years
On inspection road breath part on, patient can show chronic, thick, mucoid rhinorrhea since childhood. Examination usually shows mucosa nose Which pale And swollen, secretion mucopurulent, and disturbance of the sense of smell. Nasal polyps are found in 30% of affected individuals. Pansinusitis chronic Which repetitive usually cause Sick head due to sinus pressure in the maxillary and periorbital areas. Symptoms usually improve with antibiotic therapy but have a tendency to recur rapidly .
Recurrent otitis media is a common manifestation of primary ciliary dyskinesia. Inspection can show membrane timpani Which interested to in with mobility the bad one or No there is none at all And effusion ear Other associated otologic disorders may include tympanosclerosis, cholesteatoma, and keratosis obturans.
Middle ear symptoms in patients with primary ciliary dyskinesia (PCD) tend to be still critical during time children, with repair only after age 18 year. By Because That, patients This must under surveillance in a way strict And specific treatment approach Possible required, especially in the treatment of persistent middle ear effusion, due to the placement of the grommet repeated exposure can predispose patients to chronic otitis and worsen the long-term prognosis.
Supporting investigation
The only one tool diagnostic definitive Which standardized is electron microscopy, which is used to visualize the ultrastructure of cilia. These respiratory cilia samples were obtained from nasal scrapings or brush biopsies.
Sinus radiography (which has largely been replaced by CT scanning) typically shows mucosal thickening, opacified sinus cavities, and hypoplastic frontal and/or sphenoid sinuses
Chest radiography may demonstrate bronchial wall thickening as an early manifestation of chronic infection, hyperinflation, atelectasis, bronchiectasis, and situs reverse (at 50% patient with ciliary dyskinesia primary). Presence situs inversus is highly suggestive of Kartagener's syndrome. Bronchiectasis occurs in the lower lobes in patients with Kartagener's syndrome and immunoglobulin deficiency, whereas bronchiectasis occurs mostly in the upper lobes of patients with with fibrosis cystic. CT scan chest resolution tall is modality that most sensitive For documenting abnormality beginning And fine in in channel breath And parenchyma lungs when compared to with radiography chest routine. Consideration should be given to this imaging technique in the early presentation of primary ciliary dyskinesia (PCD) syndrome, when chest radiography may not be sufficient. sensitive For identify process disease or when differential others are being considered.
Mucosal biopsy specimens were examined for ciliary motility with use microscope light. Quantification microscopic light for ciliary pulse frequency, coordination, and amplitude, although only available in a few centers, can identify ciliary dyskinesia in patients with normal ultrastructure. Light microscopy alone offers a reliable and simple method to rule out primary ciliary dyskinesia, but combined light and electron microscopy provide a higher degree of accuracy.
Management
Kartagener's syndrome represents a diverse clinical spectrum of patients; therefore, treatment must be tailored to each patient. Continuous clinical follow-up is one of the best ways to provide type maintenance individual This. Prevention decline lung function is objective end main treatment clinical. Antibiotics, Good intravenous or orally and continuously or intermittently, used to treat upper and lower respiratory tract infections. 9,10
Tympanostomy tubes are needed to reduce conductive hearing loss and recurrent infections. Many patients undergo repeated tympanostomy tube placement, which is often complicated by suppurative otitis media. chronic. Otitis media chronic Possible need action special for ear hygiene, such as routine otomicroscopy, acetic acid irrigation, or culture-guided topical or systemic antibiotic therapy. Because of anticipated long-term middle ear disease, inserting a tympanostomy tube is the most reasonable method of maintaining the microtomy. Because tube the can endure in membrane timpani more longer compared to regular grommets. 9,10
When sinus disease cannot be managed with medical management, sinus surgery is indicated. endoscopy functional can cause repair temporary on upper and lower respiratory tract symptoms. The procedure to create an antral nasal window below the inferior turbinate may have a role in the management of primary ciliary dyskinesia because it relies on gravity rather than ciliary mucus clearance. 9,10
Definition And Epidemiology
Keratosis obturans was first described by Toynbee in 1850 who described it as a whitish mass in the posterior part of the external acoustic meatus which at that time was called molluscum contagiosum. Then in 1874 the term keratosis was finally used. obturation. 11,12 Estimate incident from keratosis obturation is four up to five patients in every 1000 new otology cases. 13,14 Keratosis obturans is more common in the younger population, namely less than 40 years. 15
Keratosis obturans is a buildup of desquamation of the keratin layer. on meatus acoustician external (MAE), colored white like pearl and form a lump that causes a feeling of fullness in the ear accompanied by hearing loss. Keratosis obturans does not cause bone necrosis and the lesion is limited to the MAE. 15,16 The tympanic membrane may appear normal or thickened and retracted. 15

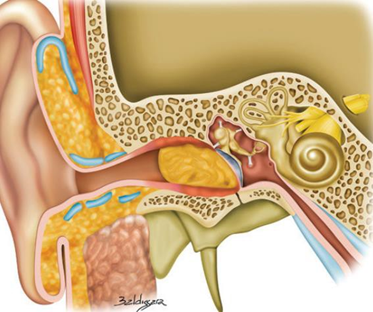
Gambar 1. Anatomi telinga17
Gambar2. Keratosis obturans pada MAE1
Etiopathogenesis
Etiology from keratosis obturation This Still Not yet clear, until moment This There is a hypothesis that has been put forward regarding the formation of keratosis obturans. Keratosis obturans can due to by a number of factor among them production excessive from cells epithelium, failure migration cell epithelium And self-cleaning mechanism Which does not work as should be. Self-cleaning mechanism on MAE is the result of the keratin maturation process and cell migration where in keratosis obturans this mechanism does not function properly. 15
Keratosis obturans is often associated with eczema, seborrheic dermatitis and furunculosis. The occurrence of keratosis obturans is characterized by the presence of an inflammatory process and increased vascularization (neovascularization) in the MAE. As a result of this inflammatory process, it also affects the tympanic membrane and layer epithelium on MAE, Where will found existence Thickening. 15 Inflammation cause improvement desquamation skin on MAE And inhibiting the migration of the epithelial layer. Under normal conditions, the surface epithelium of the tympanic membrane from the pars flaccida will migrate to the pars tensa and move inferiorly across the tympanic membrane, but the movement of the epithelium in keratosis obturas does not occur in accordance with this normal process. 15,19 Migration failure coupled with obstruction to the migration process caused by the accumulated keratin layer causes more accumulation of epithelial debris in the inner part of the EAC. 15 Accumulation of laminar keratin in the EAC is the most common form of desquamation in keratosis obturans. 15
The existence of lump keratin on MAE Which No handled with Good will be able to cause an increase in pressure on the MAE wall so that the MAE wall experience dilation And in a way No direct pressure This can causing bone remodeling around the MAE. This MAE dilation occurs slowly. This change is also accompanied by inflammation of the epithelial layer, as well as thickening of the tympanic membrane but in a condition that is still intact. 12,15
In 1965 it was reported that there was a relationship between keratosis obturans and bronchiectasis or sinusitis where both could be found in patients with a percentage of 77% in pediatrics and 20% in adult patients. This was explained in patients with sinusitis and bronchiectasis there was an increase in reflex stimulation of the sympathetic nervous system which influenced the increase in production of cerumen glands causing hyperemia and epidermal blockage. It is not explained whether the stimulus to these glands causes migration disorders 13,15,16,20 .
Classification
There is two type keratosis obturation, that is type inflammation And type silent. In the first type, the inflammatory type, there is an infectious process, such as a viral infection, as the underlying mechanism. In this type, epithelial migration is temporarily disrupted by the inflammatory process. The treatment for this inflammatory type is by extracting/removing the keratin clog that blocks the MAE. 13,14
Type Which second is type silent Which due to by migration keratin Which abnormal without existence process infection. Type This will leading on recurrent disease progression even after MAE clearance. Regular MAE clearance is necessary in the management of this type because of local metabolic deficiencies that affect normal migration mechanisms. 13,14
Histopathology
Histopathologically, keratosis obturans appears as a thickening of the epithelial and subepithelial layers showing a combination of blood capillary dilation and chronic inflammatory cell infiltration, especially in the medial part of the MAE. 12,15,21
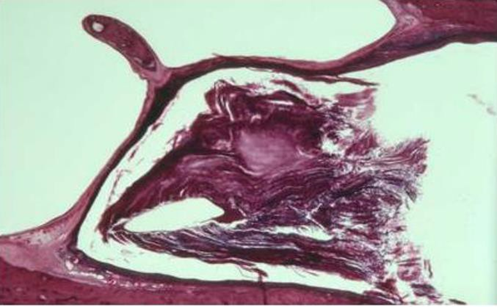
Figure 3. Horizontal section shows the inner MAE which closed by keratin squamous Which congested (hematoxylin eosin, 30x). 15,21
In keratosis obturans the keratin layer peels off in the MAE area where the older layer will be pushed to the middle, and so on until finally producing a lamellar layer (a layer that is like onion skin) which as a whole composed of layers of keratin Which congested. Inside there are layers shaped sheet congested Which similar like leaf as well as material orthokeratotic keratinosis with very little epithelial lining. 15.21
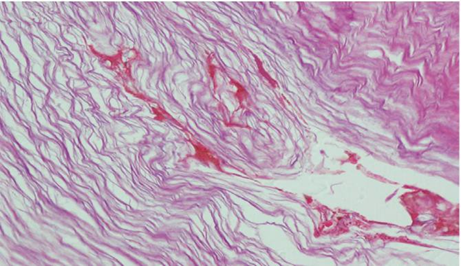
Picture 4. Fragment keratin laminar acellular (hematoxylin-eosin, 400x) 13
Diagnosis
Keratosis obturans is more common in younger population, i.e. under 40 years old, bilateral hearing loss in the form of conductive deafness, severe ear pain, tinnitus. In addition, signs of hyperemia can be found. And dilation MAE, membrane timpani Which thicken However Still in intact condition. Otorrhea is rarely found in keratosis obturans. All these signs and symptoms occur secondary to the accumulation of keratin in the MAE. 12,13,15

Picture 5. Keratosis Obturans on MAE. 15
The diagnosis of keratosis obturans is made based on anamnesis and physical examination and other examinations. In the anamnesis, severe pain in the ear, hearing loss, namely conductive deafness which is usually bilateral, and otorrhea are very rare. 15 It should be suspected in patients with cerumen impaction with characteristics that are difficult to extract with several attempts. 13
On otoscopic examination there is an accumulation of whitish keratin debris clumps in which there is brownish serum, membrane. timpani Which thicken However Still intact. Inspection Rinne And Weber can also be performed with a 512 Hz tuning fork to determine the presence of conductive deafness and then compared with audiometric examination. 15
In histopathological examination, keratin clumps are seen which form geometric lines that look like the layers of onion skin. Meanwhile, imaging examination in the form of CT-scan is only performed to determine whether there is There is whether or not erosion bone. 15 On inspection This can found lesi network soft Which Can happen in a way bilateral with location is limited to MAE, there is widening of MAE without any signs of bone erosion. 15
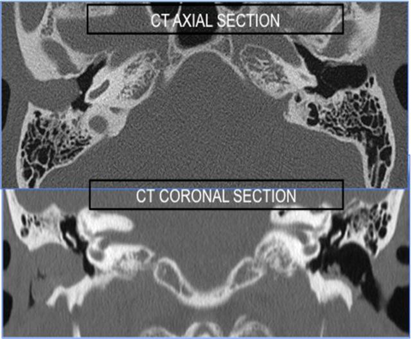
Picture 6. CT scan from keratosis obturans 15

Figure 7. Axial CT scan of the soft tissue window. show existence mass network
soft (arrow) occupy MAE, bulging membrane timpani, without erosion bone, local dilatation in lesion 18
On a study immunohistochemistry on keratosis obturation showed the presence of cytokeratins (CK 5, 6, 8, 17, 19) and tenascin. Meanwhile, growth factors EGFR, TGF beta 1, antigen Ki67 And Antigen P53 Which responsible for bone resorption was not found. 12
In addition to the above, patients also need to undergo a thorough examination because keratosis obturans is also associated with other diseases such as bronchiectasis or sinusitis. 12
Diagnosis Appeal
Keratosis obturans needs to be differentiated from cholesteatoma because it has a similar clinical picture but has a different management. The characteristics of cholesteatoma are lesions formed by keratinized squamous epithelium in the temporal bone, the most affected parts are the inferior and posterior parts of the wall. MAE bone. 15 Therapy of cholesteatoma depends on from severity disease. Therapy conservative can done when cholesteatoma and erosion bone still limited on MAE. 15
Keratosis obturans is more commonly found in younger patients with severe acute ear pain and usually also found hearing loss in the form of bilateral conductive deafness. Meanwhile, cholesteatoma mostly occurs in older patients, is generally found unilaterally, there is otorrhea, and chronic dull pain in the ear as consequence secondary from invasion network squamous to area periostitis local at MAE 5. Hearing is mostly still within normal limits. 15
On ear examination, keratosis obturans shows MAE filled with keratin plaque. After extraction, MAE will appear dilated and hyperemic due to the pressure of keratin clots on MAE. Whereas in cholesteatoma, there is diverticula epidermal Which originate from wall lower MAE, however in part MAE Which other looks normal. 15 Differentiate keratosis obturans and cholesteatoma is quite difficult because the patient's clinical signs and symptoms often overlap. overlap. So it is necessary to carry out supporting examinations others, such as imaging to find the presence of osteonecrosis or not and immunohistochemical examination to support the diagnosis. 12 Osteonecrosis and bone sequestration cannot be found in keratosis obturans but will be found in patients with cholesteatoma. 15
TREATMENT
Treatment of patients with keratosis obturans is by cleaning the MAE from the squamous epithelial layer that has peeled off 5 . Therapy can be done conservatively by cleaning the MAE and followed by follow-up. up periodically. 12 Keratosis obturation can be controlled with regular cleaning of the MAE every one to three months to reduce debris accumulation. 12 Often the diagnosis of keratosis obturans can be made after cleaning the MAE and removing the whitish matrix. In the process often cause painful Which great And bleeding as due to the peeling of the matrix in MAE due to neovascularization in it. 13
Drug drops ear with mixture alcohol or glycerin in peroxide 3% three time in a week can help For therapy 5 . A number of type drops Other ear drops can also be used to soften and remove earwax, including oil-based ear drops (eg olive oil), water-based ear drops (eg sodium bicarbonate or water), and non-water, non-oil-based ear drops (hydrogen peroxide-urea compounds). 22 There was no significant difference between the types of ear drops, all of which were effective. 22
Sodium bicarbonate ear drops have side effects such as dry ears and a mild stinging sensation. Non-aqueous, non-oil ear drops (eg, hydrogen peroxide-urea drops) can cause discomfort in the ear, increased pain, temporary hearing loss, Dizzy And tinnitus. On use drops ear Which made from olive oil base, patients may experience side effects of itching or stinging sensation and mild deafness for a while. 13,22
Ear drops containing hydrogen peroxide are contraindicated for patients with damage to the tympanic membrane, pain, otorrhea, inflammation, infection and tinnitus within 2-3 days after irrigation. For oil-based ear drops, it is contraindicated for patients with allergies, tympanic membrane perforation, ear infection, eczema of the outer ear or seborrheic dermatitis. There are no contraindications for sodium bicarbonate ear drops. 13.22

Picture 8. Clot keratin Which thick mixed with earwax which was taken from MAE after the 13th operation process
Local corticosteroids can also be used and have an important role in reducing inflammation 5 . In addition, surgical intervention can also be performed with anesthesia general For debridement Because painful Which very great as well as For patients Which No cooperative. 13,15,23 For cases Which refractory, skin graft method and canaloplasty method can be used 13 . After MAE is cleaned, it is recommended to cover MAE with gauze moistened with antibiotics and corticosteroids to reduce inflammation. 15
Complications
In general, keratosis obturans rarely causes serious complications. However on case Which heavy, keratosis obturation can cause extensive bone erosion including automatoidectomy but no intracranial complications were found 5 . The plug of squamous keratin clots can enlarge and press on the bone MAE so that cause reabsorption. 15 Patient Which have keratosis obturation Which repetitive during five year or more can causes pressure on the posterior MAE bone wall and mastoid wall which can lead to automastoidectomy. 15

Figure 9. Secondary automatoidectomy due to keratosis obturans 15 In addition That, there is A case Which report the occurrence paralysis
facial nerve. This is caused by keratosis obturans which is left untreated and eventually presses on the area around the MAE so that disorders can occur. on nerve fascialis. 16,24,25 Although is condition benign, keratosis obturans can result in resorption bone Which wide with involvement intratemporal soft tissue structures. 25 To rule out other possible causes such as Bell's palsy, herpes shingles, otitis media, Lyme disease, Guillain-Barre syndrome, sarcoidosis, Sjogren's syndrome, tumors and stroke, it is necessary to conduct a detailed anamnesis and clinical examination followed by radiological and histological examinations. 24
REFERENCE
Tadesse, A., Alemu, H., Silamsaw, M., & Gebrewold, Y. Kartagener's syndrome: A case report. Journal of Medical Case Reports , 2018. 12 (1). https://doi.org/10.1186/s13256-017-1538-2
Ciancio, N., de Santi, MM, Campisi, R., Amato, L., di Martino, G., & di Maria, G. Kartagener's syndrome: Review of a case series. In Multidisciplinary Respiratory Medicine (2015: Vol. 10, Issue 1). BioMed Central Ltd. https://doi.org/10.1186/s40248-015-0015-2
Peters, R., & de Jonge, G. Kartagener's syndrome: situs inversus, chronic sinusitis and bronchiectasis. JBR-BTR ,.2016; 100 (1). https://doi.org/10.5334/jbr-btr.955
Mishra, M., Kumar, N., Jaiswal, A., Verma, A. K., & Kant, S. (2012). Kartagener's syndrome: A case series. Indian Lung , 29 (4), 366–369. https://doi.org/10.4103/0970-2113.102831
Shapiro AJ, Zariwala MA, Ferkol T, Davis SD, Sagel SD, Dell SD, et al. Diagnosis, monitoring, and treatment of primary ciliary dyskinesia: PCD foundation consensus recommendations based on state of the art review. Pediatr Pulmonol . 2016 Feb. 51(2):115-32.
Cho DY, Hwang PH, Illek B. Characteristics of chloride transport in nasal mucosa from patients with primary ciliary dyskinesia. Laryngoscope . July 2010. 120(7):1460-1464.
Knowles MR, Daniels LA, Davis SD, Zariwala MA, Leigh MW. Primary ciliary dyskinesia. Recent advances in diagnostics, genetics, and characterization of clinical disease.Am J Respir Critic Care Med . 2013 Oct 15. 188(8):913-22.
Yue, Y., Huang, Q., Zhu, P., Zhao, P., Tan, X., Liu, S., Lee, S., Han, X., Cheng, L., Li, B., & Fu, Y. (2019). Identification of pathogenic mutations and investigation of the Notch pathway activation in Kartagener syndrome. Frontiers in Genetics , 10 (JUL). https://doi.org/10.3389/fgene.2019.00749
Sha, Y. W., Ding, L., & Li, P. (2014). Management of primary ciliary dyskinesia/Kartagener's syndrome in infertile male patients and current progress in defining the underlying genetic mechanisms. In Asian Journal of Andrology (Vol. 16, Issue 1, pp. 101–106). https://doi.org/10.4103/1008-682X.122192
Romdhoni, A. C. Keratosis Obturation Management. Biomolecular and Health Science Journal , 2018; 1 (1), 75. https://doi.org/10.20473/bhsj.v1i1.8212
Piepergerdes JC, Kramer BM, Behnke EE. Keratosis obturans and external auditory canal cholesteatoma. Laryngoscope 1980; 90: 383–391.
Shaha KK, Patra AP, Das S. Keratosis Obturation: Reviews Article. Sch J Appl Med Sci Sch J App Med Sc 2018; 6: 2215–2216.
Alarouj H, AlObaid F, AlBader AK, et al. A Recurrent Misdiagnosed and Maltreated Case of Keratosis Obturans. Case Rep Otolaryngol 2019; 2019: 1–4.
Saniasiaya J, Nik Othman NA, Mohamad Pakarul Razy NH. Keratosis obturans complicated with facial nerve palsy: a diagnostic dilemma. Braz J Otorhinolaryngol 2020; 86: 130–132.
Romdhoni A. Keratosis Obturans Management. Biomol Heal Sci J 2018; 1: 75–78.
Glynn F, Keogh IJ, Burns H. Neglected Keratosis Obturans Causing Facial Nerve Palsy. J Laryngol Otol 2006; 120: 784–785.
Moore et al. Moore Clinically Oriented Anatomy Eighth Edition. Wolters Kluwer Health, 2018.
Tsuno NSG, Tsuno MY, Neto CAFC, et al. Imaging the External Ear: Practical Approach to Normal and Pathologic Conditions. Radiographics 2022; 42: 522–540.
Corbridge RJ, Michaels L, Wright T. Epithelial Migration in Keratosis Obturans. Am J Otolaryngol - Head Neck Med Surg 1996; 17: 411–414.
Morrison AW. Keratosis Obturation. J Laryngol Auto 1956; 70: 317–321.
Naiberg J, Berger G, Hawke M. The Pathological Features of Keratosis Obturation and Cholesteatoma of the External Auditory Canal. Arch Otolaryngol 1984; 110: 690– 693.
Burton MJ, Doree C. Ear Drops for The Removal of Ear Wax. Cochrane Database Syst Rev; 2018. Epub ahead of print 2018. DOI: 10.1002/14651858.CD004326.pub3.
Myla S, Varsha K. Clinical Study of Keratosis Obturans. Clin Study Keratosis Obturans IAIM 2021; 8: 28–31.
Poudyal P, Nepal G, Yadav SK, et a. Keratosis obturation: A rare cause of facial nerve palsy. Clin Case Reports 2022; 10: 1–5.
Singh A, Truth M, Handa K. A Wolf in Sheep's Clothing: Keratosis Obturation Causing Facial Nerve Palsy - A Case Report with Review of the Literature. Turkish Arch Otorhinolaryngol 2019; 57: 102–104.
Comments