MICROTIA
I Made Nudi Arthana
Microtia is a congenital hypoplastic malformation of the auricle that ranges in severity from a fully formed auricle with subunits Which A little more small until No existence leaf ear And lobule completely, known as anotia 4 .The global prevalence of microtia has shown significant geographic and ethnic variations. Microtia widely affects approximately 3-5 children in 10,000 live births. 3 Microtia has been associated with many syndromes and is thought to be caused by vascular or drug other Which used during time development embryology. Malformation or No existence ear outside can cause disturbance hearing conductive and psychosocial, thus affecting the quality of life of the child in the future. Collaboration between plastic surgeons, an ENT specialist in otology as well as an ENT specialist in reconstructive facial plastics is required when considering the timing of repair if these two conditions coexist 4 .
LITERATURE REVIEW
Anatomy Ear Outside Normal
The ear is divided into outer, middle, and inner parts (Figure 2.1). The outer and middle parts are primarily concerned with transferring sound to the inner ear, which contains the organs for balance as well as hearing. The tympanic membrane (eardrum) separates the outer ear from the middle ear (Figure 2.1). Tube pharyngotympanic (auditorium tube) connect ear middle to the nasopharynx. 1 The external ear consists of an elegant three-dimensional cartilaginous framework with soft tissue lobules. 8
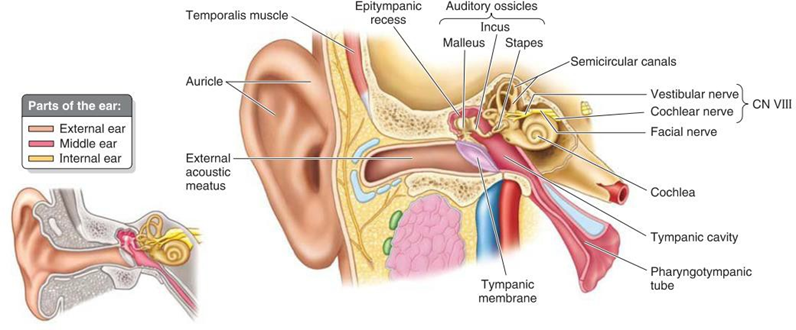
Figure 2.1 Anatomy parts of the ear 1
When reviewed in a way embryological, ear middle And outside is derivative from the first and second pharyngeal arches. The auricle is made up of several protrusions or hills on the first and second arches known as auricular hillocks. Every hillock contribute on part certain from pinna, And hillock Which there is in the arch second to form part big leaf ear. Development hillocks usually happen slowly during a number of month, with layer ectoderm on own role important in form end leaf ear. In contrast, the inner ear has a completely different embryological origin, by Because That structure ear in always normal on patient with microtia/anotia. 3 The outer ear consists of the auricle (pinna), which collects sound,
and the external acoustic meatus (EA), which conducts sound to the tympanic membrane (Figure 2.1). The auricle consists of elastic cartilage covered by skin thin. Leaf ear own a number of part Which depression And elevated. The concha is the deepest part of the depression, and the raised edge of the auricle is called the helix (Figure 2.2 and Figure 2.3). A lobule that is not composed of cartilage (earlobe) consists of fibrous tissue, fat, and blood vessels. The earlobe is easily punctured to take small blood samples and insert earrings. 1

Picture 2.2 Anatomy ear outside 1

Picture 2.3 Anatomy ear outside 8
The tragus is a tongue-like projection that overlaps the opening of the EAC. The arterial supply to the auricle is derived primarily from the posterior auricular artery and the superficial temporal artery (Figure 2.4). Venous outflow is via the postauricular vein to the external jugular system. Lymphatic drainage follows embryology with derivative arch pharynx First flow through parotid nodes and derivatives of the second pharyngeal arch via the cervical nodes. 1.8
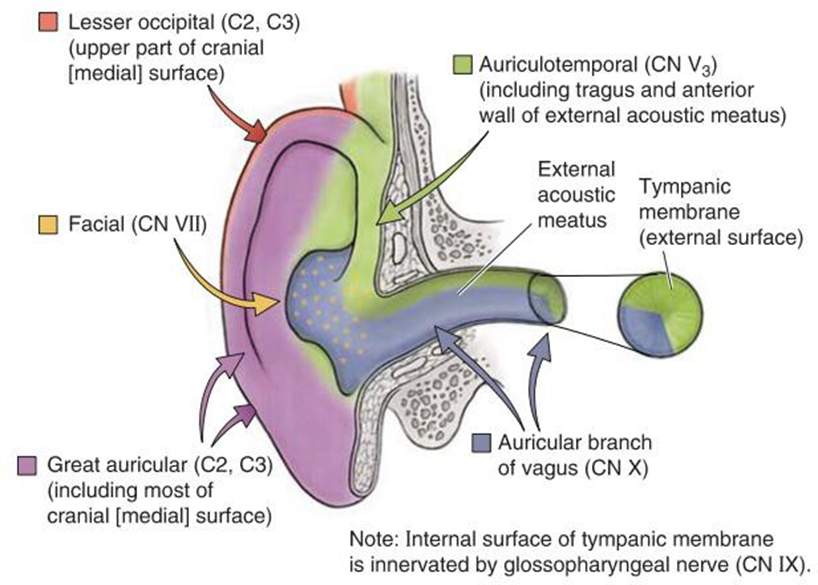
Nerve main on skin leaf ear originate from great auricular (C2-C3) and auriculotemporal nerves (cranial nerve V3) (Figure 2.5) with a small contribution from facial nerves (nerve cranial VII) And vagus nerves (nerve cranial X). 1

Skin on surface front attached close And sebaceous. Skin on posterior aspect or cranial more loose And generally bare. Share structure
into three levels or three complexes helps analyze the necessary components For make it return; level Which most cranial is conchal bowl complex, followed by antihelical-antitragal complex, And final helical rim- lobule complex. 8
The proportions and relative position of the ear to the face, jaw, and scalp are important in planning reconstruction. The height of the ear is approximately equal to its distance from the lateral eyebrow at the level of the helix root. Its width is approximately 55% of its height. Part above it parallel with eyebrows, And end lobular parallel with columella. The adult ear is usually 5-6 cm long. The helical rim projects approximately 2 cm from the skull at an angle of 21-25°. The long axis of the ear is not parallel to the nasal dorsum but is rotated posteriorly approximately 15-20° from the perpendicular axis of the body (Figure 2.6).

Picture 2.6 Dimensions and proportion of outer ear 8

Figure 2.7 Aesthetic measurement of the earlobe
A study by Otto et al. of patients with lobular microtia showed that the affected ear had less than half the surface area skin Which owned by ear Which Healthy. Imaging plaster ear model with computed tomography (CT) scan micro or CT cone beam, And Then converting the images into a mesh model, the researchers determined that healthy, adult-sized ears in the study had an average total skin area of 47.3 cm2; compared with an average of 14.5 cm2 for ears with microtia. 8
Microtia
Definition Microtia
There is various definition microtia Which proposed. Microtia in a way literally means small ears. Microtia is a spectrum of earlobe anomalies that range from remainder bone vulnerable Which No regular Which attached on lobule network soft to complete absence of the ear (also called anotia). 3 UK national guidelines define microtia as a deformation of the ear that can vary in severity from a barely present ear to a fully formed ear that is smaller than the other ear. 5 Zhang et al. (2019) in the International Consensus define microtia as a term used to describe a smaller and usually deformed earlobe. Another definition expressed 4 is that microtia is a congenital hypoplastic malformation of the pinna that ranges in severity from a fully formed earlobe with slightly smaller subunits, to complete absence of the earlobe and lobule in its most severe form, known as anotia.
From the various definitions outlined, it can be concluded that microtia is a deformation, malformation, or deformity of the earlobe that can vary in severity, from an ear that is almost absent to an ear that is perfectly formed but smaller than the other ear.
Classification Microtia
Complex malformations such as microtia require a standard classification to facilitate further understanding. A review of the literature reveals several classifications for microtia starting with Marx's classification in 1926. And ended with classification by Hunter et a. on year 2009 (Table 2.1). Most classifications depend on the surgical approach, and partly on the morphology and embryologic development. The Weerda classification is currently the standard for describing microtia. 3 The widely adopted classification system, originally developed by Weerda, then simplified by Aguilar, grades microtia from I to III based on the severity of the deformity (Figures 2.7 and 2.8). 12
Table 2.1 Variety classification microtia. 3
Grade I: earlobe with normal structure, but smaller than normal Grade II: abnormal earlobe with some identifiable features Grade III: rudimentary ear
Degrees IV: anotia
![]()
Type 1: Anonymous
Type 2: Ear Which truly hypoplastic (microtia)
With atresia canal acoustician external
Without atresia canal acoustician external
Type 3: Hypoplasia of the middle third of the auricle Type 4. Hypoplasia of the superior third of the auricle
Ear narrow ( cup and lop ears ).
Cryptoptia
Hypoplasia of the entire superior third Type 5. Prominent ear
Malformation degrees First: Part big structure leaf ear normal can
recognized (deformity minor).
Macrotia
Abnormalities form tragus And antitragus
Ear stand out ( Protruding ears )
Colobomata
Cryptoptia
Deformity lobule
No existence helix part on
Cup ear deformities
Stahl ear
Second degree malformation: Some normal auricle structures can be recognized. For example, small ears ( mini ears ).
Third degree malformation: No normal auricle structures can be seen. recognized. Classified as unilateral or bilateral. Anotia falls into this category.
Type lobule: Remainder leaf ear And lobule; without concha, canal acoustician
external, And tragus
Type concha: Level presence lobule, concha, canal acoustician external, tragus,
incisura tragic varies
Type concha small: Remainder leaf ear And lobule with curve small which represents the concha
Anotia: No or only a slight resemblance of an auricle remains Atypical: Cases that do not fall into any of the above classifications
Microtia, First Degree: Presence all components ear normal and long
median longitudinal more from 2 SD in lower average
Microtia, Second Degree: The median longitudinal length of the ear is more than 2 SD below the mean with the presence of some, but not all, normal ear structures. Microtia, Third Degree: The presence of some auricular structures, but not all none of these structures correspond to recognized components of the ear
Annotation: No existence ear The same very

Figure 2.8 Classification degrees microtia 12
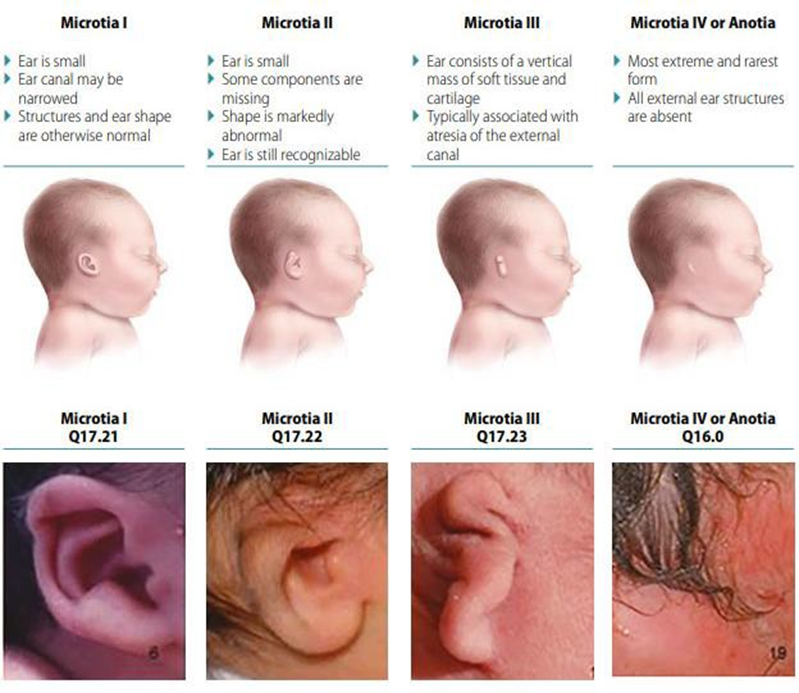
Figure 2.9 Classification degrees microtia 6
Based on the illustrations in Figures 2.7 and 2.8, grade I describes an ear that is slightly smaller than a normal ear with basically normal features. Grade II represents an earlobe that is not fully formed and deformed, but has some components that are still recognizable. Degrees III manifest as ear "peanut land" (peanut ears), with lump small network deformity Which often contain some cartilage, and grade IV is the complete absence of the ear (anotia). 12
Another frequently cited classification system was proposed by Nagata, who categorized microtia according to the vestigial structures present, into lobule-type, konka-type, small konka-type microtic ears, And anotation. Ear microtia Lobule-type microtic ears have residual ear lobes and lobules, but lack the concha, acoustic meatus, and tragus; this type usually corresponds to Grade III according to the Aguilar classification. Conchae-type microtic ears ears) have a number of lobule, concha, meatus level acousticus, tragus, and incisura tragica; this type usually corresponds to Grade II according to the Aguilar classification system. Small concha-type microtic ears contain a remnant of the ear and a lobule with a small notch for the concha. 12
Epidemiology of Microtia
External ear anomalies are common and occur in 5% of the population. The prevalence of microtia in the United States is 2-3/10,000 births, with greater increases observed in Hispanics and Japanese. In California, through a population-based study of the California Birth Defects Monitoring Program, the prevalence of microtia was found to be 2.5 million live births and stillbirths from 1989-1997. The prevalence is estimated to be 2.5/10,000 live births and stillbirths. Syndromic microtia (microtia as part of another syndrome) has been reported to be higher than isolated microtia with 1.53/10,000 birth compared to with 0.63/10,000 birth. Found also that Hispanics and Asians are more likely to have microtia/anotia compared to Caucasians. Data from the Texas Birth Defects Registry showed a prevalence of 2.86/10,000 live births with an increased incidence among Hispanics and older maternal age. A study in China revealed a prevalence of microtia of 1.4/10,000 births. An interesting finding by Castilla et al. who reported a higher prevalence of microtia along with other craniofacial anomalies in high altitude areas in Latin America. At altitudes above 3000 feet in Ecuador, the prevalence of microtia was reported 17.4/10,000 birth. Besides That, studies latest on year 2016 by
Stoll et al. in France determined the prevalence of microtia anotia in 387,067 births with a ratio of 3.77/10,000 births. 3
Microtia is usually unilateral (in 77-93% of cases), more frequently found in side right (60%), And more often happen on man (2.5:1). Prevalence per
10,000 births in The United States ranges from 1.8 to 3.5; and worldwide from 0.4 to 8.3. Based on studies in the United States, there is a risk of microtia that higher in between patient Asia, Archipelago Pacific, And Hispanic.
Previous studies of the global prevalence of microtia have shown significant geographic and ethnic variation. Although it is widely reported to affect approximately 3-5 in 10,000 live births, higher frequencies have been noted in certain ethnic groups such as the Navajo population (12 per 10,000 births) and 8.8 per 10,000 births in Chile. Studies have shown a male predisposition with a 40% higher risk for microtia, and a predominantly unilateral phenotype with the right ear more frequently affected than the left. 7
Studies on the prevalence or incidence of microtia cases in Indonesia have not been widely published, resulting in very limited data collection to create an epidemiological picture.
Etiology And Risk Factors Microtia
Ear development is complex, involving tissues derived from the neural crest as well as the endoderm, mesoderm, and ectoderm layers to form the inner, middle, and external ear. The external ear develops from the ectoderm layer and specifically arises from the pharyngeal arch. arch) First And second, Which to form six hillock of Hix at 6 weeks of gestation (Figure 2.9). While researchers have debated the exact contribution of the hillocks to the final shape of the auricle, research latest show that arch pharynx First (mandibular arch or cartilage Meckel) bring up hillock 1st until 3 And to form tragus (1), helical crus (2), And helix (3). Antihelical crura (4), antihelix (5), And lobule-antitragus complex (6) formed from arch pharynx second, Which Also known as the hyoid arch or Reichert's cartilage. 4

Figure 2.10 Theory of embryological development of the human auricle. (A) Lateral view of a native embryo. (B) Close view of the auricular hillock as explained by His in 1885.
(C) A simplified version of the auricular hillocks. Numbers 1-3 have been described as the origin of the first pharyngeal arch. And 4-6 as derivative (derivative) from arch pharynx second. (D) Theory Which proposed on the embryological development of the human auricle as described by several authors. The final development of the hillocks is as indicated by numbers 1-6. The first arrow represents the dorsal rotation of the second pharyngeal arch as described by His in 1885. The second arrow represents rotation ventral arch pharynx First like Which explained by Wood-Jones And I-Chuan in 1934. 11
Importantly, the stapedial artery also arises from the second pharyngeal arch, and if it degenerates too early, microtia can result. Eventually, these six hillocks fuse to form the auricle by 22 weeks of gestation. The auricle develops to 85% of its adult size by age 5 years and is fully developed by age 8 years. This early development is why some surgeons will choose to perform reconstruction microtia on patient Which aged very young, especially If they do not use autologous rib grafting. 4
While microtia can occur in isolation, it is sometimes associated with genetic craniofacial syndromes such as Goldenhar, Treacher Collins, Nager, Crouzon, and CHARGE syndromes, Pierre-Robin sequence, and hemifacial microsomia, oculo-auriculo-vertebral spectrum (OAVS). Teratogens, including isotretinoin, thalidomide, alcohol, and mycophenolate mofetil, when used during pregnancy or conception, can also cause microtia. Other risk factors found to be associated with microtia include maternal parity. (first mother parity) or parity tall (high mother parity), age advanced in mother or father, altitude (above 8,200 feet), and low birth weight. 4.9
A number of studies observational based on population in a way extensive investigate the possibility risk factors that associated with microtia/anotia. The risk factors reviewed are generally due to either maternal disease or exposure to certain drugs during pregnancy. High maternal or paternal age, multiple births, and maternal type 1 diabetes are among the risk factors that have been identified. A study in Japan by Okami et al. found a significant association between microtia and gestosis, maternal cold, spontaneous abortion, and anemia in 592 patients with microtia. Several epidemiological studies have associated Hispanic race and high altitude with the occurrence of anotia/microtia. Low birth weight Also associated with microtia, although No found connection causality between the two. Exposure to retinoids, thalidomide, and mycophenolate mofetil is strongly associated with microtia/anotia. It was later found that up to 49% of microtia cases are associated with other anomalies or syndromes, although the percentage varies widely in previous literature ranging from 20-60%. Non-syndromic congenital malformations involving the heart, kidneys, and facial skeleton including facial clefting, and asymmetry have also been reported with varying percentages. Several other studies have shown an association of microtia with aberrations of chromosomes 13, 18, and 21 with percentages ranging from 2-14%. Linkage to chromosome 18 is the most commonly reported. These findings encourage the search for other possible syndromes, in order to provide optimal treatment. 3
Pathogenesis Microtia
The exact pathogenesis of microtia is still poorly understood. Embryological review allows for a better understanding of the pathogenesis of microtia. The anatomy of the microtia ear is similar to the anlage seen in embryo 6 Sunday. Microtia is common associated with atresia or absence of the external auditory meatus, indicating developmental delay. The accepted theory is that the external and middle ear develop from the first (mandibular) and second (hyoid) pharyngeal arches. The auricles begin to develop on age pregnancy five Sunday from six hills, three in second side of the first branchial cleft between the two arches, which becomes the external canal. On Finally, hillock from arch First contribute on development tragus and root of the helix , and the remainder of the auricle develops from the hillocks of the second arch. Ossicles ear middle develop from arch First And second with The mastoid air cells, eustachian tube, and remainder of the middle ear develop from the first pharyngeal pouch. Membrane timpani develop in where first bag meet with the first gap. 8
Initially, the ear has a ventromedial position, which becomes more dorsolateral as the midface and mandibular processes grow and push it outward and upward. Interruptions in the proliferation or fusion of the hillocks at various stages of fetal development may produce diverse rudimentary structures that appear as microtia. 8
Diagnosis Microtia
In diagnosing microtia, anamnesis, physical examination, and comprehensive supporting examination are required. The doctor must ask about the patient's medical history. complete patient including infection ear, development talk And language, and family history of hearing loss and ear anomalies. 9
A complete physical examination of the infant should be performed to look for associated syndromic findings. 9 In some cases, microtia is associated with genetic syndromes, and therefore examination and notation of syndromic features should be documented as well as inspection for hemifacial microsomia, pre-auricular pits, complement auricular accessories, And atresia aural. Inspection size
The ear can be a major step in the physical examination. A fully developed normal human ear is about 6 cm tall, tilts 20 degrees back from the vertical, and has an auriculocephalic angle of 20-30 degrees with a distance of 2-2.5 cm from the edge of the helix to the mastoid. Microtia is a condition in which there is underdevelopment of the ear; in some cases, only part of the lobule and helix are present. Which seen. Moment inspect patient, important For do complete head and neck examination that includes evaluation of the mandible, oral cavity and palate, eyes, facial nerve function, skin color and quality, temporoparietal hairline level, And position remainder leaf ear. Component leaf ear ear should be examined and compared with the contralateral side. 4 It is also important to monitor the middle ear status in the apparently healthy ear to ensure optimal hearing is maintained for the ear with better hearing. 9
Various supporting examinations are recommended in cases of microtia, these examinations include hearing examinations and CT scan imaging, 9 which are discussed as follows:
Inspection Hearing
When a baby is born with microtia, the affected ear will usually fail in newborn hearing screen (NHS). Regardless from results NHS, baby should be referred directly to an audiologist for outpatient diagnostic Auditory Brainstem Response (ABR) testing. Newborn hearing screening is mandated and performed universally in the United States, but often by non-medical volunteers. Regardless of the presence or absence of an ear canal, infants with microtia or severe auricular malformations should be referred to a pediatric audiologist (or a general audiologist who do sleep ABR) for diagnostic hearing test. 9
Diagnostic ABR testing should be performed as early as possible. Diagnostic ABR testing should include at least thresholds for broadband stimuli such as clicks or CE-Chirp, as well as tone burst thresholds between 500 Hz and 4,000 Hz. Air conduction and bone conduction testing should be performed. In particular, masked bone conduction testing will isolate response cochlea the ear that affected with Good, For ensure
bone conduction response actually originates from the ear being tested. In the case of atresia channel bilateral, only unmasked bone conduction Which can measured due to inability For cover response conduction bone with appropriate. If no, in case stenosis or atresia channel ear unilateral, test masked bone conduction must done For ear Which affected. Besides That, tympanometry should be done (tympanometry 1000 Hz For show mobility eardrum And tympanometry 226 Hz For confirm volume channel ear) and distortion product otoacoustic emissions on ear with channel ear patent. 9 In most infants from birth to 6 months of age, diagnostic ABR
this can done moment baby currently Sleep without sedation (Picture 2.10). In on age six month, evaluation audiologist must done with use method developmentally appropriate behavioral tests (visual reinforcement audiometry, conditioned play audiometry, standard audiometry). Behavioral audiological evaluation is essential to determine hearing thresholds (via masked bone conduction) For ear with microtia/atresia as well as ensure And monitor hearing sensitivity for non-microtia/atresia ears. Children who have difficulty assessing behaviorally may require ABR with sedation. Sensitivity hearing on population This must monitored every year or two times a year until the age of 5 years. 9

Picture 2.11 Baby undergo ABR without sedation (natural sleep). 9
In cases of microtia, patients should be referred to audiology as early as possible. Diagnostic audiology assessment should be completed by 2-3 months of age and infants should be fitted with hearing amplification by 4 months of age and enrolled in early intervention by 3-6 months of age to optimize speech and language development. 9
CT Scan
CT scan of the temporal bone is not recommended in the newborn period. born. Inspection This must done moment before option surgery Hearing reconstruction is proposed (approximately at age five, depending on surgical plans) or If There is concern will cholesteatoma. Inspection CT A high-resolution scan of the temporal bone without contrast is recommended before any microtia reconstruction to assess candidacy for atresia repair and to rule out the presence of a congenital middle ear canal or cholesteatoma (Figure 2.11), although Possible No required If family The same very not interested in atresia repair. Attention clinical for cholesteatoma, often seen in cases with severe canal stenosis, may require diffusion-weighted imaging (DWI) magnetic resonance imaging (MRI) to help confirm the diagnosis. Renal ultrasonography in the newborn period may be performed to rule out renal abnormalities associated with the cause of microtia syndrome. 9

Picture 2.12 Description CT scan stenosis canal acoustician external with cholesteatoma. (A) Coronal and (B) axial sections without contrast. 9
Management of Microtia
Comprehensive management of microtia involves counseling and education of parents, provision of hearing aids, and surgical reconstruction which will be discussed further as follows:
Counseling And Education Person Old
Newborns should ideally be referred to an audiologist and otolaryngologist for consultation regarding the child's hearing status. In addition, referral for genetic testing is recommended if the child appears to have a particular syndrome at birth. These referrals can be made on an outpatient basis, although many parents feel comfortable seeing an ear, nose, and throat (ENT) specialist after birth, especially for hearing problems. An adolescent with hemifacial microsomia may require surgical referral. plastic or surgery mouth And maxillofacial related hypoplasia mandible and problems malocclusion. Person old or patient Which want information more more about reconstruction microtia Which Actually must referred to to expert surgery microtia which experienced; including expert surgery plastic/expert surgery craniofacial, expert pediatric ENT, or expert surgery plastic face. Evaluation For delay talk And language and early intervention should be recommended to parents of children with developmental delays and disabilities, including isolated hearing loss.9
Person old from baby new born with microtia Possible experience strong emotional turmoil, especially guilt and frustration. It is important to counsel parents about the theoretical causes of microtia, the impact on hearing, And Then guide they related choice For hearing and reconstructive surgery. In fact, in most cases, the cause of microtia is unknown. Self-blame by parents should be minimized as much as possible. Advising parents on how to talk to the affected child, friends, acquaintances, or other family members about the patient's "small ears" is also very important to prevent feelings of embarrassment. Families should be encouraged to seek out support groups or online communities and forums to minimize feeling isolated and give example positive about how children with microtia can grow into healthy and productive adults. 9
Giving Tool Hearing Aid
Children with microtia are most often found to have conductive hearing loss (CHL) on the side of the ear with microtia. Hearing loss is confirmed at the time of diagnostic audiology evaluation. Amplification options for children with microtia can be either nonsurgical or surgical. Before age five year, options non-surgical amplification is recommended, as few surgical implant device options are approved for use. by Food and Drug Administration (FDA) American Union for kids aged five year to above. 9 Approach non-surgical And surgery further explained as follows:
Approach Non-Surgical Giving Tool Hearing Aid
Various tool hearing aid available For help children with CHL which is related with microtia (Picture 2.12). Bone conduction sound processor (BCSP) such as the Cochlear BAHA® or Ponto can be worn on an accessory called a softband. Another option is the Med-El ADHEAR sound processor, which can be worn on adhesive gel pads or a special soft band. In children over the age of five, the Cochlear BAHA® SoundArc can be used in conjunction with the Cochlear BAHA® Sound Processors and worn on the back of the head instead of a headband. 9

Figure 2.13 Non-Surgical Bone Conduction Device (Bone conduction sound processors). (A) Cochlear BAHA® with soft band. (B) Ponto® with soft band.
(C) Med-El ADHEAR® with bearing gel adhesive. (D) Cochlear BAHA SoundArc®. 9
Doctors should encourage early use of these bone conduction devices for infants with CHL. In cases of bilateral microtia, the infant may already be fitted with the device. by audiologist on age 4 month. On patient with microtia unilateral, where the non-microtia ear has normal hearing, it is important to consult a pediatric audiologist to discuss the choice of bone conduction device and encourage its early use for early adaptation to use. tool help hear. Although children in lower age three year rarely exposed to challenging listening environments, the experience of most audiology centers is that the successful use of bone conduction aids in children age school correlated with installation And adaptation previously. Parent must given know that they Possible No see difference behavior on installation beginning tool help conduction bone, And a number of person Possible feel that matter the No give difference. Objective installation beginning is adaptation to amplified sound for sensory integration into the child's experience in preparation for school age. 9
Parents should be informed that there may be challenges regarding protection. insurance For tool help hear conductive bone on patient with microtia unilateral. They Also must given know that age toddler can be a challenge in successfully using the device, and a target of 2–4 hours of use per day is recommended until the child is more tolerant of longer use. Many programs have a minimum target for daily hearing aid use while in school. 9
Approach Surgery Giving Tool Help Hear
Once patients reach the age of five, they are candidates for bone conduction sound processors (BCSP) with an osseointegrated implant retention system that is surgically placed using subcutaneous magnets or percutaneous abutments (Figure 2.13). These implants allow children to use bone conduction sound processors without softbands or adhesive gel pads. 9

Picture 2.14 Devices conduction bone with approach surgery. (A) Cochlear BAHA® with osseointegrated percutaneous abutments. (B) Ponto® with buffer And screw For osseointegration. (C) Cochlear BAHA ATTRACT® with subcutaneous magnet. (D) Med-El BoneBridge® with magnet subcutaneous. (E) Cochlear OSIA® with magnet subcutaneous. (F) Magnetic implants by Medtronic. 9
Type buffer (BAHA® Connect, Ponto) And system magnetic (BAHA® Attract, Medtronic Magnetic Implant) have similar osseointegrated implants in the skull, but each allows the sound processor to connect to the implant differently. The percutaneous abutment is placed through the skin, while the magnetic system is not. 9
Overall, transcutaneous magnetic systems allow for the elimination of penetrating braces. However, hearing improvement is less than with magnets. Different magnet strengths are available to accommodate varying scalp thicknesses, although devices may become dislodged or fall out with weaker attachments. Sometimes, the scalp needs to be surgically made thinner to accommodate the magnetic attachments. 9
On the contrary, buffer percutaneous allow conduction bone directly without lost vibration in skin. Buffer percutaneous Also offer more secure attachment of the processor to the implant, which may be beneficial for active children in park play. However, interface buffer skin prone to to reaction local skin complications such as recurrent infections and skin overgrowth. The complication rate of percutaneous abutments requiring revision surgery was as high as 44.4% percent; with the risk of implant loss ranging up to 25% in pediatric patients. 9
Active implants with direct bone conduction without skin penetration (Osia®, BoneBridgeTM) are currently FDA approved for patients 12 years of age and older. However, successful implantation has been reported in younger patients both in and outside the United States. This method provides optimal hearing amplification without penetrating the skin. These devices also rely on a transcutaneous magnetic system to connect microphone external. However, transducer delivery person bone is a component that is implanted under the skin. This allows microphone separation And component active tool help hear, remove problem bait come back Which normal found, without lost amplification in all over skin head or problems with skin complications. 9
After discussing the choice of hearing aids that are fitted through approach surgery, furthermore is How determine candidate implantable hearing aids and the appropriate timing of surgical implantation. Close consultation with the audiology team and family is essential to determine a patient's candidacy for surgical implantable hearing aids. A child with a history of poor compliance with softband hearing aids, for example, may not be a good candidate for an implantable device, especially if the patient does not benefit from the device, does not like the sound, or does not want to wear any device that might attract attention. A child who is a good candidate for ear canal reconstruction may not want to proceed with an implantable device.9
Regarding the optimal timing of implant placement surgery, surgeons placing osseointegrated implants for hearing management must work closely with expert surgery reconstruction so that operation implant No compromise fascial flaps or skin that may be important for microtia repair. It may be preferable to place an implant after microtia reconstruction, although coordination Which Good allow For merge procedure Ear reconstruction and hearing augmentation. 9
If implant placement is to be performed prior to microtia reconstruction, the implant should be placed in the posterior temporal region. It is essential to maintain the vascular integrity of the superficial temporoparietal fascia during implant placement. Doppler examination of the superficial temporal artery at the time of surgery is recommended for safe placement of the implant posterior to the vascular pathway (Figure 2.14). If a patient and family desire repair microtia Not yet consult with expert surgery microtia, or have not yet decided the timing and type of approach desired, delaying hearing aid implant surgery may be prudent so that all operations can be coordinated later. 9

Figure 2.15 Surgical markings indicating the course of the superficial temporal artery. (line intermittent), place main tool help hear conduction bone And implant "sleeper" (white arrow) 9
If a non-surgically fitted, adhesive prosthetic ear is desired, some osseointegrated hearing implants can be placed at any time after age five year. If prosthetic surgically installed planned (e.g. Vistafix®), reconstructive surgery and implant placement can be performed simultaneously. 9
If families choose alloplastic ear reconstruction, osseointegrated hearing implants can be placed at the same time as alloplastic ear reconstruction surgery or three months after the ear has healed. For autologous cartilage repair, implants can be placed at the same time during the surgical stage where the newly created ear is removed, allowing access to the back of the ear through the same incision. Alternatively, osseointegrated hearing implants can be safely placed three months after the final stage of autologous cartilage repair. 9
Surgery Reconstruction Microtia
When discussing the spectrum of reconstructive options, there are three general modalities available, namely leaf prosthesis ear, alloplastic porous polyethylene , and autologous cartilage reconstruction. 9 These three modalities are discussed further as follows:
Prosthesis earlobe
Realistic silicone ear prostheses can be made for individuals of all ages (Figure 2.15). Elderly people who want ear prostheses generally look for help moment child aged between four And five year, or school age. The appropriate time to consider initiation of prosthetic use is the developmental age at which a child is able to care for and comply with the use of the prosthetic. Depending on the location of the ear microtia, an ear prosthesis can be fabricated to cover the ear and provide the desired symmetry with the contralateral ear, using Computer-Aided Design and 3D printing. Anaplastologists factor in future tissue growth for the adhesive-supported prosthetic to ensure proper and secure maintenance. The anaplastologist then carefully paints the prosthesis to match the skin. This expertise and skill are essential For satisfaction patient. Ear prosthetic Also can made For covering ear reconstructions that produce poor cosmetic results. No surgery is required for these adhesive prostheses, thus delaying the option for more invasive interventions until the patient is mature enough to participate in the decision-making process. 9

Picture 2.16 Prosthesis silicone ear compared to with the contralateral ear healthy . 9
Osseointegrated implants placed surgically can allow for more secure prosthetic attachment using clips, snaps, or magnetic attachments, and can be implanted after age 5. anaplastology must involved in planning surgery Because location The implant is critical to the success of the prosthetic outcome. Some patients may experience chronic inflammation around the percutaneous abutment, similar to those who experience buffer percutaneous osseointegration For BCSP. Put implants and/or excision of the external ear will have serious consequences, including inhibiting repair. in time front on reconstruction microtia. For reason This, patient must be mature enough to participate in the decision-making process. 9
A successful prosthesis must fit properly and be secure enough to be worn all day without worry. The prosthesis can be pierced with earrings and allows for the use of eyeglasses, oxygen tubing, hearing aids, and face masks. Other considerations include the potential need to remove the prosthesis during contact sports and swimming. Prosthetic ear care includes appointment on Evening day before Sleep And cleaning every day.
Prosthesis Which made with Good must endure two until three year And remade with installation new For take into account change network soft. There may be some discoloration over time and degradation of the thin clear prosthesis margins. 9
Parents should be informed that ear prostheses provide the appearance of a normal external ear with the psychological benefits of symmetrical, realistic ears without the risks of surgery. Concerns about the prosthesis falling out No on purpose can influence image self a child. Matter the can be overcome by counseling and comparing artificial ears with other commonly used health devices such as glasses and hearing aids. 9
Reconstruction ear with alloplastic porous polyethylene (PPE).
Alloplastic reconstructions, such as Medpor® and SuPor®, use a high-density porous polyethylene implant covered with a well-vascularized fascial flap, usually the temporoparietal fascia flap (TPFF), which is then covered with residual temporoparietal skin and graft. skin (Picture 2.16). Reconstruction alloplastic usually done as a one-stage operation. Alloplastic reconstruction can be performed from the age of three. Early repair is considered to have a positive psychosocial impact, that when the microtia ear is repaired before the child starts school, he/she does not have to worry about being bullied by other children. Early reconstruction emphasizes the importance of agreement child For operation elective big Which change life. Improvements in quality of life have also been reported following alloplastic reconstruction. 9

Figure 2.17 Alloplastic reconstruction. (A) Temporoparietal fascia flap (TPFF) is raised. (B) Porous polyethylene (PPE) auricle framework. 9
Profit Which most interesting from reconstruction alloplastic is that the reconstruction is performed in one stage, and the age at the time of surgery does not depend on the child's growth and size, as in cartilage reconstruction. Loss from reconstruction alloplastic including risk extrusion, fracture, and infection. Some people find this is amplified because the alloplastic reconstructed ear is numb. Without sensation in the PPE earlobe, the risk of injury, infection, And extrusion can increase And in progress lifelong life. If extrusion does occur, the TPFF, which is often used for salvage in autogenous cartilage reconstruction, has been exhausted in the initial repair. However, other fascial options such as the occipital artery flap may be used in salvage surgery. When the vascularity of the reconstructed ear is dependent on a single vessel in the pedicled fascial flap, pressure may affect its viability, as it does during sleep. From the patient's perspective, sleep comfort may be an issue to overcome. Some children can sleep with special pillows around the ears to relieve this pressure. 9
When reconstruction Alloplastic ears are performed on children of a younger age, so the PPE earlobe created will be larger than the contralateral ear. This is because healthy ear growth in the future needs to be taken into account. Therefore, patients and families must be informed and agree to the difference size beginning This, when reconstruction alloplastic done For child the younger one. 9
Cases in which alloplastic reconstruction may be most beneficial is in case microtia bilateral, reduce amount operations and symmetry problems, and for children who are very young for age (such as children with certain syndromes), which otherwise require a high degree of patient willingness. wait until the time teenagers, in order to have a stock of cartilage that Enough For reconstruction Which adequate later. On children with hairline Which its location low, except done disappearance hair with laser, then this reconstruction technique is less useful. This is because TPFF is obtained from that area. Other conditions in which alloplastic reconstruction is beneficial is on person mature Which more old, Because For eliminates the risk of experiencing cartilage calcification which makes the earlobe difficult to carve. 9
Reconstruction bone autologous prone
Use of the patient's own (or autologous) ribs for reconstruction leaf ear considered by Lots person as gold standard for surgery reconstruction microtia (Picture 2.17). Action carry on during a number of decades have shown that a properly performed surgery can provide patients with a stable, lifelong reconstruction. The surgery is completed in 2-4 stages, depending on the surgeon's technique. Typically, it begins when the patient is at least six years old.

Figure 2.18 Autologous cartilage reconstruction. (A) Typical area of costochondral cartilage harvest. (B) Example subunit leaf ear made from bone vulnerable costochondral. (C) Pre-operative image ear microtia. (D) Assembly framework leaf ear costochondral. (E) Appearance postoperatively immediately after stage 1 costochondral cartilage reconstruction. 9
This surgical technique was first introduced by Tanzer, then refined by Brent to achieve acceptable autologous ear reconstruction results. A variation of Brent's 4-stage technique remains the most widely used method in the United States. With Brent's method, the smaller amount of cartilage required than other techniques allows reconstruction to begin around age six. Later, Nagata and Firmin described a 2-stage autologous approach that provides greater detail but requires a greater volume of cartilage. Which larger. Reconstruction using the technique Nagata And Firmin usually offered on age Which more old when the child has circumference chest minimum 60 cm, as indicator standard bone ribs enough . 9
Profit from reconstruction cartilage is base knowledge wide which has collected, Because use approach This in a way wide in all over world. The reconstructed ear has sensation and vascularity compared to the alloplastic ear. Cartilage reconstruction allows for the creation of an individual ear, sculpted by the surgeon, to create symmetry with the contralateral ear. This modality is ideal for many forms of microtia, especially degrees of microtia where the of the remaining ear can be saved, and part of the defect reconstructed, as in grade 2 microtia. Cartilage reconstruction allows the surgeon to reconstruct only the missing subunit of the ear, preserving the desired portion of the microtia ear, which may not be possible with alloplastic techniques. 9
Wrong One weakness from technique bone vulnerable is condition For 2- 4 stages, separated by 3-4 months, depending on the surgeon's technique. The initial timing of surgery depends on the patient's chest size and thus allows for adequate stock. bone vulnerable bone ribs Which Enough For make ear, by Because it requires a longer waiting period before surgery. There is also morbidity from the donor site at the time of surgery and scarring along the chest, although most patient No report effect side term long which is detrimental For problem on the site donor. Patient No own wall deformity chest or limitations in activity or sport in time front after taking bone vulnerable bone ribs. Complications term long Which
reported complications include framework resorption and wire extrusion, although overall, comparisons show fewer long-term complications using autologous cartilage compared with PPE. Pneumothorax is complications term short Which No normal from rib removal, and is usually easily treated and resolves without prolonging hospital stay or causing long-term consequences.9
After knowing the modalities available for microtia ear replacement, furthermore Which need under consideration is time operation And technique to be used. Several factors must be considered in determining the timing of cartilage-based reconstruction. The age, size, and maturity of the patient are important factors. Age guidelines are general, as many factors such as genetics, diet, and medical comorbidities are strong determinants of a child's size. A chest circumference of 60 cm, measured at the xiphoid level, has classically been the minimum indicator of rib adequacy. Classically, a chest CT scan is performed to evaluate the costal cartilage, allowing for visibility of synchondrosis and evidence of calcification. However, with increasing awareness of exposure radiation on children with CT scan, matter This become not enough Good in daily practice. Recently, cartilage ultrasonography (USG) has been reported to accurately assess rib dimensions without the need for ionizing radiation exposure. Multidisciplinary evaluation and careful discussion with the child and parents also help determine psychological and anatomical readiness. 9
There are key moments in the timeline for hearing improvement. And reconstruction on children. Recommendation age intervention for children's hearing needs are explained as follows 9 :
Baby new born: Screening hearing
1–3 month: Sleep deprived ABR
6–9 month: Behavioral audiogram
3–6 months: Consultation about hearing aids (bilateral cases must fit with a softband device at 4–6 months of age)
12 months-5 years: testing audiology and supervision every 6-12 months
5 year: Consider CT scan For installation implant hearing.
Consider waiting for surgery to implant a bone conduction device until after or at the same time as concomitant microtia reconstruction. Consider the Cochlear™ BAHA® SoundArc mode or adhesive gel for use with a bone conduction sound processor.
Recommendation age intervention For reconstruction microtia explained as follows 9 :
Baby New Born: Consultation with expert surgery reconstructive for parental counseling regarding future reconstructive options
3–5 year: Age most beginning For consideration reconstruction Alloplastic PPE .
5 years: Earliest age for osseointegrated anchor for prosthetic use. Prosthetics can be used with adhesives before the age of 5 years.
5–9 year: Age most early For reconstruction autologous cartilage .
Another consideration besides the surgical time is surgical expertise. Either technique, alloplastic or cartilage reconstruction, requires a high level of surgical expertise with experienced surgeons to achieve reliable results. Surgeons performing microtia reconstruction should perform the surgery regularly and have advanced training. 9
There are three main techniques used in autologous cartilage reconstruction for microtia reconstruction, which are commonly used in variations tailored by the reconstructive surgeon (Table 2.2) 9 , these techniques are discussed further as follows:
Table 2.2 Stages from technique general reconstruction autologous 9
Technique | Stage 1 | Stage 2 | Stage 3 | Stage 4 |
Technique Traditional Brent | 1) Costal cartilage removal 2) Framework creation earlobe 3) Inserting the framework into the retroauricular skin remainder microtia | Lobules are diverted to the framework remnants of microtia | Elevation ear and posterior auricle skin graft placement |
|
Technique Brent Modification | 1) Costal cartilage removal 2) Making a framework with strut strut 3) Inserting the framework into the retroauricular skin remainder microtia | Lobules are diverted to the framework remnants of microtia | Elevation ears plus costal cartilage covered with fascia flap and graft skin | N/A |
Nagata/Firmin | 1) Retrieval | 1) Ears elevated | N/A | N/A |
| costal cartilage 2) Making the framework intact 3) Inserting the framework into the retroauricular skin 4) Lobule transposition , inserting the framework into lobule | 2) Elevation plus curved costal cartilage , covered with facial graft and graft skin |
|
|
N/A, not available
Brent Technique
The Brent technique was the first modern microtia technique to gain widespread popularity as adapted from Tanzer. This technique is traditionally accomplished in 4 stages as follows 9 :
Stage 1: Retrieval bone vulnerable costa 6th until 9th And forming the ear frame. The cartilage frame is then placed into a subcutaneous pocket at the ear reconstruction site.
On phase First reconstruction, frame ear got from costal cartilage contralateral from ear Which reconstructed. Incision horizontal made above limit costa, muscle oblique external And muscle rectus separated. The ear template is placed on the costal cartilage as a guide to how much cartilage costa Which required. Cartilage costa Which used For The helical rim is taken from the first floating rib and is separated from the main ear. The synchondrotic region of the 6th and 7th ribs is made up of the body from framework ear. Dissection supraperichondrial made For
preservation specimen And reduce possibility deformity chest wall .
Brent performed preservation at the upper border of the 6th rib cartilage. During fabrication of the ear frame, the helical rim and antihelical complex details were exaggerated due to the overlying skin. will be blunt cover the details of region This. Brent recommend anticipation framework ear into a curve. For the helix part, the curve forms a flexion so that it can be attached to the ear frame. The helix is sewn with nylon 4.0 in the horizontal direction.
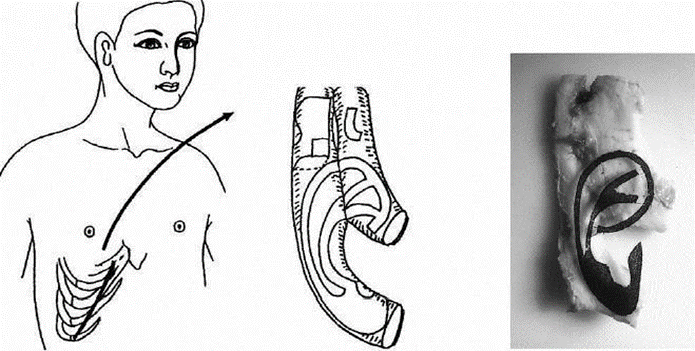
Figure 2.19 Costal cartilage removal

Figure 2.20 Framework creation ears of cartilage ribs
Stage 2: Lobule transposition in the second phase to prevent scar tissue formation, reduce circulation and elasticity and reduce the risk of tissue necrosis.

Stage 3: The ear is elevated using a skin graft placed on the posterior aspect of the ear and advancement of the retroauricular skin.
Sulcus formed by elevating the reconstructed ear from the scalp and covering it with a full thickness skin graft. In this step, it is necessary to after details auricle Already seen And edema Already disappear. The incision is made a few millimeters behind the rim and the auricular skin should be advanced so that the auricular part Which need graft is part posterior ear. Full thickness Skin grafts are taken from the lower abdomen or inguinal fold.

Picture 2.22 Elevation framework and plant skin until to the sulcus
Stage 4: tragus construction and concha excavation and simultaneous contralateral otoplasty.
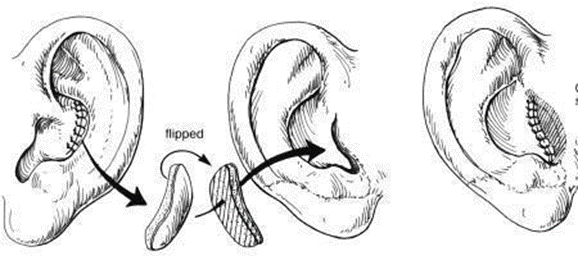
In the next phase Brent constructs the tragus, creates the concha and forms the artificial meatus, and elevates the reconstructed auricle away from the head. The tragus is formed by taking a composite chondrocutaneous graft from the anterior surface of the contralateral ear concha. Brent then places it under a J-shaped incision in the region of the reconstructed ear concha. The straight part of the J incision then becomes the boundary marker of the tragus while part arch from incision J earlier will become intertragal notch. The concha is deepened with emit network soft under the plant tragus. When removing soft tissue behind the tragus flap, the tragus will form a shadow that can resemble a meatus.
Picture 2.23 Tragus construction
More recent modifications to the Brent technique have reduced the number of stages to three by combining tragus formation in the first stage, framing the tragus, and often combining the final stage with placement of an osseointegrated hearing implant. 9
Technique Nagata/Firmin
Satoro Nagata is figure Which revolutionize reconstruction leaf ear with a 2-stage technique, in which tragus reconstruction and lobule transposition are both performed in the first stage. Françoise Firmin went on to describe what many consider to be a modified Nagata technique, characterized by skeletal projection cuts and a formal classification of the skin approaches which she called Types 1, 2, 3a and 3b. This technique provides approach standard For reconstruction leaf ear Which take into account remainder microtia And contour Which is lost For reproduced. This technique uses autologous costal cartilage to reconstruct the ear in 2 stages as follows 9 :
Stage 1: The 6th to 9th costal cartilages are harvested and carved to create a framework that encompasses all ear structures that need to be reconstructed, including the tragus. The cartilage framework is then placed deep into the residual retro- and peri-auricular skin with concomitant lobule transposition. Degrees microtia Which different need variation in skin approach .
Stage 2: Ear elevation is performed by incising the skin around the frame. Bone vulnerable addition placed in posterior For projecting the ear. This is obtained through a second harvest or comes from excess cartilage that is stored in the soft tissues of the chest at the time of the first operation. In this technique Nagata, cartilage Which used For postauricular elevation The sulcus is covered with vascularized TPFF and skin graft.
Firmin describes four techniques for elevating the ear and recreating the retroauricular sulcus, which he categorizes as Type A elevations. Type A is the standard Nagata technique that utilizes the TPFF fascia to provide vascularization to the elevated cartilage. Type B is the Brent technique, in which no cartilage is used, the posterior ear is elevated. And closed with graft skin, And skin retroauricular brought forward. Type C describes the use of random fascia derived from the posterior mastoid region, which is inverted to provide vascularization to the elevated cartilage, then covered with a skin graft. Type D is known as the tunnel technique, where a tunnel is created in the soft tissue covering beneath the skeleton, then a block of cartilage is placed to support the ear forward. Because these are tunnels, they do not require coverage with a facial flap. The retroauricular sulcus is then closed with a skin graft. The elevation technique chosen depends on patient factors such as the degree of projection of the other ear, the hairline, and the amount of cartilage available for the second stage. 9
The advantage of the 2-stage technique, although it requires a larger cartilage framework, is that the ear is reconstructed with greater detail and depth. However, this technique is more dependent on skin conditions and can result in improvement risk complications wound like area small dehiscence and postoperative skin viability issues. These complications can usually be managed with maintenance or closing wound local. Profit from technique Brent is every stage allow skin For healed in between the stages, thus reducing the risk of wound complications. 9
Complications Microtia
In addition to the general risks of surgery including pain, bleeding, swelling, infection, scarring, damage to surrounding structures, and the need for For surgery more carry on, complications repair microtia including pneumothorax from costal cartilage harvest, cartilage infection (often with Pseudomonas aeruginosa), extrusion of the cartilage framework, changes in framework size, lobular necrosis, and migration of the construct from its original location. Compression ischemia with loss of skin and temporoparietal fascia flap is also an early complication of porous polyethylene implantation. Facial nerve injury may occur due to the lack of a predictable anatomical pathway in the underdeveloped ear. In addition, prosthetic ears are easily misplaced, and replacement costs are high. 4
Construct extrusion usually occurs above the superior helical edge and is treated by covering with a temporoparietal fascia or occipitoparietal fascia flap . Complications This is complications Which most often need a return to room operation for repair Because helix superior tend to have the weakest blood supply in the reconstructed earlobe. 4 Construction cartilage costa And implant polyethylene porous can migrate or shift after placement, usually to anteroinferior, although determine location Which appropriate For placement beginning Also Can very challenge. Many cases microtia accompanied by hemifacial microsomia, Which make use of side normal face as template not enough help. Although generally stand long in term long, polyethylene porous own potential to be extruded or infected with relatively little trauma compared to autologous cartilage constructs.4
Lastly, most patients will have a low hairline on the side of the microtia. Matter This can cause skin head retainer hair cover the reconstructed upper part of the ear, which may later require laser removal. 4
Prognosis Microtia
The prognosis depends on the outcomes measured and which treatment approach is chosen. Bone-anchored hearing aids can be applied to treat conductive hearing loss very well, and in some cases, the leaves ear microtia can hidden with hair long. Thus Also, the application of the prosthesis creates an ear that allows the patient to avoid social scrutiny and can serve as a support for glasses. In an article by Chunxiao et al. on patient satisfaction after microtia reconstruction with autologous cartilage, patients were most satisfied with the helix and least satisfied with the tragus appearance. However, the relatively high complication rate with autologous cartilage reconstruction makes preoperative counseling essential for management of expectations and satisfaction. patient Which more Good. Part big patient on Finally satisfied with their reconstructed earlobes, especially since many felt that construction the become part from they, different with how patients often view ear lobe prostheses. 4
Overall, the prognosis for hearing outcomes from bone conduction devices is reliable, has fewer surgical risks, and is usually better than outcomes from ear canal reconstruction. However, they are dependent on patient compliance and have psychosocial impacts. from usage tool help hear. Devices conduction bone passive imposed on soft band (BAHA®, Ponto) can offer average tone pure similar to that worn with implanted magnets (BAHA Attract®). However, implanted active bone conduction devices (Osia®, BoneBridgeTM) give strengthening frequency tall Which more Good. With better high frequency retention, patients can obtain better speech discrimination scores with active bone conduction implants compared to passive bone conduction devices.9
DISCUSSION
Microtia is a congenital abnormality characterized by malformation or deformity of the earlobe that can vary in severity, from almost nonexistent ears to fully formed ears that are smaller than the other ear. Microtia is often a non-isolated abnormality but is associated with other syndromes. Most occur unilaterally, but as many as 10% are bilateral. A study in China disclose prevalence microtia 1.4/10,000 birth. Findings more by Castile et a. Which report prevalence microtia which more tall along with other craniofacial anomalies in Latin America.
Microtia can occur at any time during embryonic development, and the type of microtia that occurs depends on when the embryonic development occurs. Several population-based observational studies have extensively investigated possible risk factors associated with microtia/anotia. Risk factors that generally considered to be due to either maternal disease or exposure to certain drugs during pregnancy. High maternal or paternal age, multiple births, and type 1 diabetes in the mother are Wrong One factor risk Which has identified. A studies in Japan by Okami et a. find from 592 patient with microtia show significant association between microtia and gestosis, maternal cold, spontaneous abortion, and anemia. According to Alnujaim in 2017, there was an association between microtia and aberrations of chromosomes 13, 18, and 21 with a percentage ranging from 2-14%. The association with chromosome 18 is the most common.
According to Troung et al, 2022, in diagnosing microtia, anamnesis, physical examination, and comprehensive supporting examination are needed. The doctor should ask for a complete history of the patient including ear infections, speech and language development, and family history of hearing loss and ear anomalies. A complete physical examination of the baby should be performed to look for findings related syndromes. Examination size ears can be
The main steps in the physical examination. Andrew in 2023 stated that when examining a patient, it is important to perform a complete head and neck examination that includes evaluation of the mandible, oral cavity and palate, eyes, facial nerve function, skin color and quality, temporoparietal hairline level, and position of the remaining auricle. The auricular components of the ear should be examined and compared to the contralateral side. It is also important to monitor the status of the middle ear in the apparently healthy ear to ensure optimal hearing is maintained for the ear with better hearing.
Inspection support is a matter Which important done to diagnose patient micronia, a number of inspection Which can done such as, hearing examination and CT scan. The examinations performed include BERA. BERA will help measure the response to sound stimuli that are recommended to accurately determine the degree of hearing, whether it is a conductive or sensorineural disorder. CT scans are used to describe the anatomy in more detail in the middle and inner ear. 10
Management comprehensive microtia involving counseling And education to parents, provision of hearing aids, and surgical reconstruction. Counseling And education to people old is a basis Which important, This greatly affects the success of a doctor in providing treatment to patients with microtia. Evaluation for speech and language delays and early intervention should be recommended to parents of children with developmental delays and disabilities, including hearing loss.9 Children with microtia most often found have conductive hearing loss ( CHL) on the side of the ear with microtia. Disturbance hearing confirmed on moment evaluation diagnostic audiology.Options amplification For child with microtia can through the approach non-surgical or surgery. Before age 5 year, option amplification non-surgical treatment is recommended, as few surgical implant device options are approved for use. by Food and Drug Administration (FDA) American Union for children aged 5 years and above.
Age Which Good For done surgery reconstruction ear said on age 6 until 7 year. According to Storck year 2014, matter This depends a number of considerations are 1) the average time for ideal costal cartilage development, 2) the risk of children being bullied by peers due to ear abnormalities Which owned by him And 3) size Which relate from frame auricle formed and the contralateral normal ear. 2 It was agreed that at the age of 6 years it was made target intimidation by Friend same age so that child Also motivated for more cooperative undergo operation. On age 6 until 7 year Also allows the results of the audiometry examination to be more accurate, the size of the contralateral ear approaches the adult size, the pneumatization of the mastoid bone is perfect and the calvarium Enough thick For implantation BAHA. On age minimum 5 year The size of the ear has reached 90 to 95% of the size of an adult ear. According to Olsinki, some researcher start moment child aged 10 year or moment long circumference chest reaches 60 cm.
Indication done surgery that is If child experience atresia bilaterally, the child is fitted with a bone conduction hearing aid at the earliest possible age. Child with microtyphoid atresia unilateral And his hearing normal on the ear Which No experience abnormality, No done therapy surgery as an effort to hearing rehabilitation. If the child with stenosis congenital canal, it is likely more urgent to reconstruct the canal because retained debris and keratin can form cholesteatoma. Auricular reconstruction is done before atresia surgery to prevent keloid formation. 3 Microtia is often followed by canal atresia. Contraindications for surgery on canal atresia are sensorineural deafness or middle ear abnormalities. It is also necessary to consider whether there is mastoid pneumatization And ear middle or the occurrence hypoplasia on cavity timpani And the facial nerve is not formed. In addition, it is also contraindicated if there is a decrease in the tegmen in the middle cranial fossa so that anatomically it prevents it from entering the tympanic cavity. 3
In general, there are 3 reconstruction options for microtia, namely autologous grafts , alloplastic ear frames and prostheses. Autologous reconstruction, such as the 4-stage Brent technique and the 2-stage Nagata technique using rib cartilage. For build frame auricle. On reconstruction with frame alloplastic, skeletal auricle Which used in the form of porous polyethylene (Medport). According to Troung year 2022, cartilage costa autogenous still is standard gold Graft material for auricle reconstruction. This is because its use can reduce the number of infections, easy frame formation and avoid the risk rejection body to network foreign Which enter, as well as tolerance ear against fairly good long-term pressure. According to Troung in 2022, the disadvantages of using autogenous cartilage are the complexity of the carving technique and the limitations of graft retrieval based on chest wall development. In addition, in some cases, cartilage graft absorption occurs. According to Troung, there are advantages to using alloplastic materials, namely that they are non-absorbable and easy to shape, and also reduce the level of morbidity in place donor. Vascularization Which rapid growth of host tissue and collagen deposition will increase the elasticity of Medpor implants as well reduce possibility the occurrence infection. Besides That contour 3 dimensions Accurate ear measurements were also achieved in 87.1% of cases in the study by Troung.
Surgery in cases of microtia is one of the complicated maxillofacial surgeries. Microtia abnormalities are often accompanied by canal atresia and hearing loss so that in auricular reconstruction accompanied by improving the degree of hearing with meatoplasty and reconstruction of the bone chain hearing. 4.6 Technique surgery on case microtia There is a number of type, namely technique Nagata, Park, Fisher And Brent. Nagata as much as 2 phase using cartilage autologous, Park use development network subfacial With 2 grafts , Fisher used 1 phase of the Nagata technique. The advantages of using this technique are: Nagata is creation projection ear Which Good And deformity minimal chest wall. 7 However, the disadvantages are having to take the costal cartilage twice, the risk of wire extrusion, the use of fascia grafts with blood vessels superficial cause depletion hair in place donor, use of graft fascia temporoparietal limit use of graft in the future, And tissue necrosis soft consequence transposition lobul on phase First. Use method Park promises good vascularization of the ear frame with split flap surface attachment , the ability to create a deeper conchal base, with a realistic auditory meatus and a hidden scar behind the mastoid. Whereas the drawbacks in the form of possibility congestion vein After expansion and elevation of the graft, the patient must have more frequent outpatient check-ups for the expansion process and depression of the mastoid bone secondary to pressure from tissue expansion. 7 The Fisher technique promises good aesthetic results with reduced risk of complications but has the disadvantage of requiring revision. and can lost the entire ear construction. On The Brent technique has a small complication rate of 0.25% and detailed auricular reconstruction but has the disadvantage that it is performed with many phases of reconstruction. 8
Factors that can determine the success of ear reconstruction are (1) the method used; (2) the child's age and developmental maturity. 9 Another important thing is hearing rehabilitation.
Bone-Anchored Hearing Aid (BAHA) is a hearing aid as an alternative strategy for hearing rehabilitation in microtia patients with unilateral or bilateral aural atresia, especially in patients with the type of surgical candidate with marginal or poor scores. 8 This approach uses titanium which placed in area mastoid until happen osseointegration. Osteointegration This allows for more efficient sound transfer than can be achieved with traditional bone conduction hearing aids. BAHA implantation can be performed in either a 1- or 2-stage operation. The titanium is implanted and left to osteointegrate for 4 months. The sound processor is connected after 3–6 weeks. 6
CONCLUSION
Microtia is a congenital disorder characterized by malformation or deformity on the leaves ear. Most happen unilateral, However as much as
10% can occur bilaterally. Microtia is an imperfect embryonic development disorder. Microtia is often a disorder that does not stand alone but is associated with other syndromes.
Reconstruction auricle For anomaly congenital is based on the severity of the auricular abnormality compared to the contralateral normal auricle, in unilateral cases. The classification of congenital auricular defects is clinically divided into lobular type microtia, concha type microtia, and concha type microtia. small, conchae type microtia, and anotia and low hairline. It is very important for the operator to reconstruct the auricle in a detailed 3-dimensional morphology. There are several materials for fabricating 3-dimensional ear frames, namely using costal cartilage, alloplastic and prosthesis as well as with tissue expander . Criteria for reconstruction leaf ear is patient must on age 10 year And circumference chest at the level of the xiphoid process reaches 60 cm.
There are several techniques used to make earlobes, namely: Brent , Nagata , And Park . However Which own results Which Good, stand long, and less complication is the Nagata technique with 2 stages. The first stage is fabrication and taking the 3-dimensional graft of costal cartilage and the second stage is the projection of the reconstructed auricle. It is very important to place the auricle at the projection angle, the distance between the temporal surface to the highest part of the auricle with the height of the constructed cartilage to produce a perfect and symmetrical projection.
There are complications that can occur with each technique and type. frame Which used, However each Also own its own advantages. In cases of microtia, it is also not uncommon for hearing loss to occur, so hearing rehabilitation is needed. use AIDS hear conductive implanted under the skin needs to be done. In addition, it is also necessary to consider making a new canal considering that microtia is often followed by canal atresia.
REFERENCE
Agur, A. M. R., & Dalley, A. F. (2019). Moore's essential clinical anatomy . In Moore's Essential Clinical Anatomy (6th ed.).
Alnujaim, NH, & Alnujaim, MH (2017). Review of Microtia : A Focus on Current Surgical Approaches . The Egyptian Journal of Hospital Medicine. https://doi.org/10.12816/0040136
Andrews, J. (2023). Ear Microtia. StatPearls Publishing. https:// www.statpearls.com/ArticleLibrary/viewarticle/20844
English Academy of Audiology, English Association of Audiovestibular Physician, English Association of Paediatrician in Audiology, English Association of Plastic, R. and A., Surgeons, Changing Faces, Ear, N. and T.-U. K., Microtia UK, National Deaf Children's Society, Paediatric Psychology Network UK, & Center for Appearance Research. (2019). UK Care Standards for the Management of Patients with Microtia and Atresia. https://www.microtiauk.org/wp-content/uploads/MICROTIA-and ATRESIA- CARE-STANDARDS-final-May-2019-004.pdf
Centers for Disease Control and Prevention. (2021). Congenital Anomalies of the Ear Microtia/Anotia. https://www.cdc.gov/ncbddd/birthdefects/surveillancemanual/quick reference-handbook/microtiaAnotia.html
Jovic, T. H., Gibson, J. A. G., Griffiths, R., Dobbs, T. D., Akbari, A.,Wilson-Jones, N., Costello, R., Evans, P., Cooper, M., Key, S., Lyons, R., & Whitaker, IS (2021). Microtia: A Data Linkage Study of Epidemiology and Implications for Service Delivery. Frontiers in Pediatrics, 9. https://doi.org/10.3389/fped.2021.63003 .
Lin, S. J., Kazei, D. D., Bauer, B. S., & Corcoran, J. (2021). Microtia. Medscape. https://emedicine.medscape.com/article/1290083-overview#a8
N Baluch, S Nagata, C Park, et a. Auricular reconstruction for microtia: A review of available methods. Plast Surg. 2014;22(1):39-43.
Truong, M. T., Liu, Y.-C. C., Kohn, J., Chinnadurai, S., Zopf, D. A., Tribble, M., Tanner, P. B., You, K., & Chang, K. W. (2022). Integrated
microtia and aural atresia management. Frontiers in Surgery, 9. https://doi.org/10.3389/fsurg.2022.944223
Ronde EM, Esposito M, Lin Y, van Etten-Jamaludin FS, Bulstrode NW, Breugem CC. Long-term complications of microtia reconstruction: A systematic review. J Plast Reconstr Aesthet Surg. 2021 Dec;74(12):3235- 3250. doi: 10.1016/j.bjps.2021.08.001.
Veugen, CCAFM, Dikkers, F.G., & Bakker, B.S. (2020). The Developmental Origin of the Auricula Revisited. The Laryngoscope, 130(10), 2467–2474. https://doi.org/10.1002/lary.28456
Zhang, T., Bulstrode, N., Chang, K.W., Cho, Y.-S., Frenzel, H., Jiang, D., Kesser, B. W., Siegert, R., & Triglia, J.-M. (2019). International Consensus Recommendations on Microtia, Aural Atresia and Functional Ear Reconstruction. The International Journal of Advanced Otology, 15(2), 204–208. https://doi.org/10.5152/iao.2019.7383
Comments