Nasopharyngeal Carcinoma
I Made Nudi Arthana
Nasopharyngeal carcinoma (NPC) is a rare, malignant tumor that starts in the nasopharynx, the tissue at the back of the nose that connects to the throat.
LITERATURE REVIEW
1 Anatomy Nasopharynx
Nasopharynx is A tubule musculofascial Which connecting cavity rice and oropharynx. Nasopharynx is part from pharynx Which located most superior, is located posterior to the nasal cavity, and is located between the floor of the sphenoid sinus and the soft palate 1 , 2 The nasopharynx also connects the nasal cavity to the ear middle through choanae And tube Auditive 3 . Nasopharynx is a room Which own wall superior, posterior, two wall lateral, and the inferior wall. Part front from the nasopharynx restricted by part posterior nasal And septum rice, temporary on part posterior nasopharynx restricted by the pharyngeal mucosa. Behind the pharyngeal mucosa of the posterior wall, there is the pharyngobasilar fascia and the upper part of the superior constrictor fibers that close the anterior arch. bone atlas.4 Wall superior pharynx restricted by mucosa pharynx, corpus sphenoid, and the basilar part of the occipital bone. The superior and posterior walls of the nasopharynx fuse and form a concave slope. which runs from the nasal septum to the oropharynx. The inferior part of the nasopharynx is bordered by the surface of the palate. mole Which crooked. Nasopharynx And oropharynx relate through pharyngeal isthmus. Elevation of the soft palate and constriction of the palatopharyngeal sphincter will close the isthmus during the swallowing movement. On the lateral wall of the nasopharynx is the orifice of the auditory tube (Figures 1 and 2). 5,6,7,8,9,10,11,12,13,14
In the nasopharynx there is a lymphoid tissue in the form of tonsillae pharyngealis located on the upper part of the superior and posterior walls of the nasopharynx. Tonsillae pharyngealis consists of adenoids and nasopharyngeal tonsillae. A number of structure important other Which found in nasopharynx can be found on the lateral wall. On each side of the lateral wall of the nasopharynx there is an opening of the auditory tube or eustachian tube. 4 On the posterosuperior part of the eustachian tube auditory there is A elevation mucosa Which known as torus tubarius. This elevation is formed by the cartilage of the auditory tube. Posterior to the torus tubarius, can found A fossa Which elongated to on until roof pharynx, known as fossa Rosenmüller. Fossa Rosenmuller closed by torus tubarius because the torus tubarius is larger at the superior and posterior edges of the auditory tube. 14,15
The epithelium of the nasopharynx in the anterior part is the epithelium of the respiratory tract. layered pseudo, ciliated, with cell goblet. On the surface There is an opening of the seromucous glands of the mucosal and submucosal layers. In the posterior part, the respiratory tract epithelium then changes into stratified squamous epithelium non-keratinized Which to be continued to part oropharynx And laryngopharynx. The transition zone between the two types of epithelium is composed of columnar epithelium with microvilli. Which short. On part superior, zone This meet with septum rice and on part lateral zone This pass orifice tube auditory. Fossa
Rosenmuller Also coated by mucosa nasopharynx Which consists of from epithelium pseudostratified columnar ciliated with cell goblet And is location beginning from most nasopharyngeal carcinoma 14
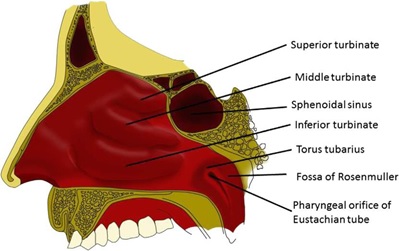
Picture 2.1 Nasopharynx from piece sagittal. 14
Picture 2.2 Nasopharynx from piece coronal. 13
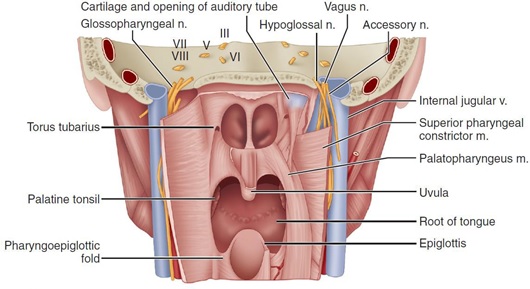
In the nasopharynx, there are several primary muscles that play a role in swallowing movements, including the tensor veli palatini, levator veli palatini, and salpingopharyngeus. All over muscle the originate from opening tube eustachian. The tensor veli palatini tenses the soft palate, while the levator veli palatini moves the soft palate upward. This movement closes the nasopharynx from the oropharynx during move swallow. Salpingopharyngeus Also help Movement swallow through elevation pharynx. Third muscle the Also open orifice tube eustachian tube during swallowing. This movement helps balance atmospheric pressure between the middle ear and the nasopharynx. 2
The nasopharynx receives its blood supply from branches of the internal carotid artery (carotid artery). mandibular), artery maxillary (artery pterygopalatine), artery facialist (ascending palatine artery), and the ascending pharyngeal artery. The blood flow then goes to the venous plexus parapharyngeal drainage towards the vein facialist And retropharyngeal vein, to Finally going to vein jugular. 2.14
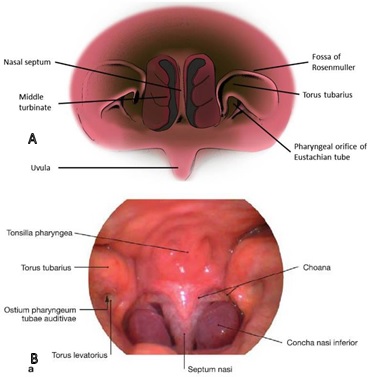
Picture 2.3 Nasopharynx from looks anterior. 14,15 A. illustration, B . picture endoscopy
Innervation nerve nasopharynx in a way main originate from plexus pharyngeal formed by the branching of the cranial nerves (CN) glossopharyngeus (IX), vagus (X), And fiber nerve autonomous truncus sympathetic. Supply innervation sensory from the membrane mucosa pharynx superior originate from CN trigeminal division maxillary (CN V2), temporary innervation motor originate from CN accessories (XI) part cranial. These nerve fibers innervate all the muscles of the pharynx except the stylopharyngeus muscle. through branch nerve vagus going to to plexus pharynx. The stylopharyngeus muscle is innervated by the glossopharyngeal nerve. 14
Drainage fluid lymphatic from nasopharynx, including Which originate from adenoids, the pharyngeal end of the auditory tube runs to the cervical lymph nodes in the superior part. The drainage can be direct or indirect through the retropharyngeal lymph nodes. And parapharyngeal. Drainage lymphatic Also walk through additional spinal KGB on triangle posterior neck. The lymphatic system of The nasopharynx can also run across the midline to the contralateral lymph nodes. 14
1 Definition of Carcinoma Nasopharynx (NPC)
Nasopharyngeal carcinoma (NPC) is an epithelial carcinoma originating from the mucosa lining the nasopharynx. This tumor is often found in the fossa of Rupenmuller. 1 World Health Organization (WHO) year 85 classify NPC into three subtypes, according to the histological picture as follows 7 :
Carcinoma cell squamous non-keratinizing ( differentiated And
undifferentiated )
- Carcinoma cell squamous keratinizing
- Carcinoma cell squamous basaloid
Keratinizing nasopharyngeal carcinoma is more common in non-endemic areas than in endemic areas such as South China (<8%), while kera ... non-keratinizing found on Part big case endemic (>95%) and is associated with EBV infection. 1,7
2 Etiology Carcinoma Nasopharynx (NPC)
Various studies moment This has show that various factor, including
Epstein-Barr virus (EBV) infection, genetic factors, and environmental factors contribute to the development of NPC.
- Factor genetics
As mentioned earlier, the incidence of NPC in the South Chinese population is higher compared to the Western countries' population. China South Which do emigration to area in American Union with the incident NPC Which low still own risk Which more tall For experience NPC compared to the native population in the United States. So it is concluded that there is vulnerability locus genetic certain in development NPC. One of the major genetic risk factors that has been identified is the human leukocyte gene. antigen (HLA) class 1 Which located chromosome 6p9 on region MHC. 1.5 Genes HLA class 1 coding protein Which identify And presenting foreign antigens, including EBV-encoded peptides, to cytotoxic T cells to trigger a host immune response against virus-infected cells. Individuals with specific HLA alleles may have a less efficient ability to trigger a cytotoxic immune response against EBV-infected cells, thus having susceptibility to NPC. The role of genes located in the HLA region on chromosome 6p9 was also found to be strongly associated with NPC in a recent large-scale genome-wide association study. 5
In addition to the HLA region, several genes also have significant associations with NPC including TNFRSF7 on chromosome 13q12, MECOM on 3q14, CDKN2A/2B on 9p9, CLPTM1L/TERT on 5p15l, And MDS1-EV on 3q14. Recent studies have shown that heterozygous pathogenic variants of the MST1R gene, which encodes macrophage-stimulating cell surface receptor 1 and is key in the body's defense against viral infections, are strongly associated with young-onset (age ≤ 8 years) nasopharyngeal carcinoma. 1,5 Case-control studies have shown an association between gene polymorphisms and risk NPC through its influence in vulnerability individual to infection EBV and/or cell transformation induced by chemical carcinogens. Increased risk NPC connected with polymorphism gene Which involved in nitrosamine metabolism (CYP2E1, CYP2A6), carcinogenic electrophile decondense (GTSM1), DNA repair (XRCC1, hOGG1, NBS1), EBV entry into nasopharyngeal epithelium (PlGR), interleukins (IL1A, IL1B, IL2, IL8, and IL10) and toll-like receptors (TLR3, TLR4, TLR10). 5
- Factor Epstein infection Barr virus
EBV infection has been associated with NPC since serological evidence has been found that NPC patients have higher antibody titers against EBV viral capsid antigens compared to healthy controls. In a cohort study, increased immunoglobulin (Ig) A and anti-DNase antibodies against EBV were reported. own association Which strong with development NPC.5 The mechanism of NPC development related to EBV infection is not fully understood, but there are several important processes that contribute to the oncogenic potential of EBV in NPC. These mechanisms include latent infection, gene expression, immune evasion mechanisms, genetic and epigenetic changes, inflammation and tissue damage. 6
Direct EBV infection of the nasopharyngeal epithelial cells is very rare, except in nasopharyngeal dysplastic lesions and non-keratinizing NPC . EBV infects B lymphocytes through its binding to the CR2 receptor on the surface of B lymphocytes. The CR2 receptor is generally rarely found or almost absent. on epithelium mucosa region head And neck. Cell Which infected by EBV can form A conjugate special cell B – cell epithelium Which involving glycoprotein GP350 of the EBV viral capsule and the CR2 receptor of B lymphocytes. These infected B lymphocytes can be found in the nasopharyngeal mucosa and adjacent to cell epithelium nasopharynx Which polarized, so that happen transmission from EBV. EBV virions can also enter epithelial cells through the basolateral membrane through the interaction between EBV glycoprotein (BMRF-2) and α5β1 integrin of epithelial cells. This pathway may illustrate the route of transmission of EBV virus from infected epithelial cells. to cell epithelium Which close together through membrane lateral. EBV Also can enter to cell epithelium through complex IgA/Sc (component secretory) Which found on the mucosal surface of epithelial cells through endocytosis. 5
- Factor environment
Previous studies reported that consumption of Cantonese salted fish in childhood was correlated with increased NPC in endemic populations. This was confirmed by an experimental animal study and found that rats fed with salted fish developed malignant nasal and paranasal tumors. Food other Which pickled or preserved Which relate with NPC in the Chinese population among others is shrimp paste and preserved vegetables. In contrast, consumption of fresh fruits and vegetables, especially during children, has reported become factor protective to NPC in the Chinese population. 5
Besides factor diet, environmental factors other like formaldehyde exposure, wood dust, smoke, And substance chemistry Also has reported as factor risk NPC. This exposure causes chronic inflammation in the nasopharynx. Smoking has also been reported as a risk factor for NPC. 13,5 The combination of alcohol consumption and smoking has also been reported to increase the risk of NPC. 6 However, the role of smoking in the development of NPC is controversial because several studies have not found an association between smoking and NPC. 6,13,5
3 Pathogenesis Carcinoma Nasopharynx (NPC)
Until now, the pathogenesis of NPC has been hypothesized to be an interaction between susceptibility gene, infection EBV And carcinogen from environment. Development NPC is thought to start from stable EBV infection in the nasopharyngeal epithelium. 6 Genetic susceptibility in high-risk populations (Southern Chinese population) in the form of HLA haplotypes and variants in the region encoding MHC I on chromosome 6p9 contribute to the increased risk of persistent infection and clonal expansion of EBV-infected epithelial cells. 7 After infecting epithelial cells, EBV will cause several genetic alterations and increase the growth of infected cells. Epithelial cells in the nasopharynx are maintained alive by telomerase. This may occur because EBV infection causes a phenotype that stops cell growth and senescence. The main trigger of NPC carcinogenesis is regulated from track Cyclin expression D1 (overexpression CCND1 or homozygous deletion of CDKN2A) and inactivation of tumor suppressor gene (TGFBR2). Dysregulation of Cyclin D1 expression contributes to facilitating persistent latent EBV infection. Propagation of EBV infection is also supported by suppression of p4 expression. These genetic alterations support the existence of EBV and facilitate cell transformation into cancer cells. 5,7
Cell epithelium Which infected EBV Also own phenotype with resilience higher survival rate compared to uninfected cells, including under conditions of nutrient deprivation. The exact mechanism of this ability is not yet clearly understood, but it is thought to involve activation of the Pl3K and Akt pathways. The resistant phenotype to stress Also observed on cell nasopharynx Which express latent membrane protein (LMP) 1. LMP1 expression inhibits the AMPK/LKB1 signaling pathway which promotes cell growth and survival. 5
EBV infection can be classified as latent infection and lytic infection. Latent infection of EBV is thought to be involved in tumorigenesis, while lytic reactivation of EBV infection in infected cells will cause cell death. EBV readily establishes type 2 latency in NPC cells and causes the expression of EBV genes, including EBV-encoded small ribonucleic acid (EBER), EBNA1, LMP1, LMP2, BART miRNA, BARF1, And EBV- encoded miRNA. The genes the involved in process tumorigenesis. Role from these genes can seen on Picture 2.4. 5 Various gene the on Finally will affect unlimited cell growth, resistance to apoptosis, mechanisms avoider immunity, inflammation Which support tumor, And genomic instability (Figure 2.5). 7 One of the genes that is important in the development of NPC is LMP1. LMP1 can cause genomic instability and stimulate the release of immune suppressive cytokines so that infected cells can evade the immune system's recognition mechanisms. LMP1 can also increase cellular mobility, invasion And metastasis KGB cervical. 6.5 In general short, activity EBV oncogenicity can be seen in the effects it has on the host genome by modifying the genetic profile, causing genomic instability, evading immune cells, and increasing cell survival through LMP1 activity. 6Cell epithelium Which infected EBV Keep going get exposure cytokines inflammation present in the tumor stroma, including tumor necrosis factor (TNF) - α, tumor growth factor (TGF) – β, Interleukin (IL) 6, IL8, And and so on. Reactive oxygen species (ROS) Which produced or secreted from cell inflammation Which active aggravate DNA damage and genomic instability of surrounding epithelial cells. Cytokines produced by inflammatory cells can also activate the NF-κB and STAT3 signaling pathways in EBV-infected epithelial cells, stimulating cell growth and survival that facilitate the transformation of infected nas cells into cancer cells. 5,6
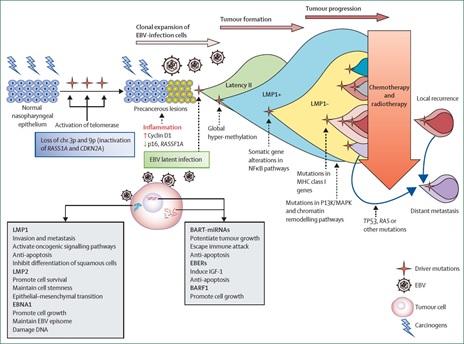
Picture 2.4 Infection EBV And Change Genomics in Development of Nasopharyngeal Carcinoma. 1
During tumor development, acquired mutations of several negative regulatory factors in the NF-κB signaling pathway alter the activity of various cancer-related genes. All these conditions increase tumor heterogeneity. Genetic changes are more carry on obtained during development tumor. On stage carry on, recurrence Local tumors and distant metastases from NPC cells after conventional treatment may be influenced by mutations in class I genes. MHC and on the remodeling pathway PI3K/MAPK And chromatin, as well as mutation somatic TP53, RACE, And other genes, 1.5
In addition to the role of EBV infection initiating tumorigenic transformation, exposure chronic mucosa nasopharynx on carcinogen from the environment increases DNA damage and causes somatic genetic changes in epithelial cells. Activation of telomerase activity on chromosomes 3p and 9p and inactivation of suppressor genes growth tumor like RASSF1A And CDKN2A will increase resilience cell, Good cell with histology Which normal and/or experience dysplasia and causes genomic instability. 1 One of the carcinogens that has been widely linked as factor risk NPC is food Which pickled And preserved. Some traditional foods from Southern China contain volatile nitrosamines. The active carcinogenic metabolites of nitrosamines can induce deoxyribonucleic acid (DNA) damage and chronic inflammation of the nasopharyngeal mucosa in susceptible populations. Consumption of these carcinogens during childhood may lead to the accumulation of aberrant genetic lesions and contribute to the development of process the emergence cancer on nasopharynx in age early, predisposes to EBV infection and increases the risk of NPC. 5 Meanwhile, habits such as smoking also increase the risk of NPC through reactivation of latent EBV infection. In the study by Cheng et al., it was found that the risk of smoking increase in a way significant ( odd ratio (OR) = 1.34; interval confidence interval (CI) 95%: 1.15-1.57) compared to never smoking. The risk is increased with improvement intensity, duration And amount box cigarette cumulative each the year. Risk NPC Also observed increase 12% - 30% in connection with passive smoking during childhood or passive smoking during adulthood. 4 Nicotine contained in cigarettes contains carcinogenic agents derived from nitrosamines that increase carcinogenesis. 8
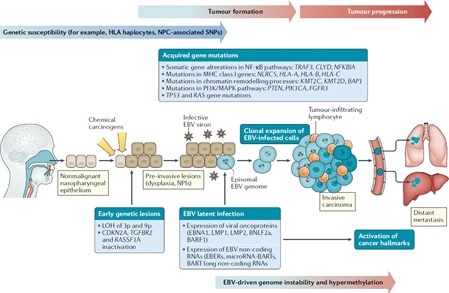
Figure 2.5 Illustration of the Hypothesis of Nasopharyngeal Carcinoma Pathogenesis. 7 Exposure carcinogen from environment can induce various lesi genetics which then becomes a predisposition for EBV infection. EBV infection triggers dysplastic lesions that eventually develop into nasopharyngeal carcinoma.
4 Manifestation Clinical Carcinoma Nasopharynx (NPC)
Sign And symptom from NPC varies And on stadium beginning often These symptoms are nonspecific, varying from asymptomatic, stuffy nose, epistaxis, to hearing loss due to middle ear effusion due to auditory tube obstruction. Signs and symptoms of NPC correlate with the anatomical region involved in the expansion of NPC, so that a thorough head and neck evaluation is needed. comprehensive required For patient with suspicion NPC. Based on the location and extent of the tumor, the signs and symptoms of NPC can be grouped as follows 1,6 :
- Common signs and symptoms: headache, fever, anemia, weight loss .
- Nasal level: unilateral nasal obstruction, epistaxis, nasal voice, decreased sharpness smell, disturbance olfactory Which varies until kakosmia heavy. Around 80% patient experience sign And symptom nasal involvement .
- Ear level: recurrent middle ear infections with ototubal dysfunction, hypoacusis due to colposis, sensation of ear fullness, otorrhea, otorrhagia, middle ear effusion, and tinnitus.
In general, at the beginning of the development of the disease, complaints often involve the ears, nose, or vision which then persist and increase in intensity over time. However, NPC patients often come with manifestations of metastasis that occur such as a unilateral mass in the neck due to cervical lymph node metastasis (50-77%). In this condition, clinically there may be no clinical manifestations of nasopharyngeal tumors. In about 54.2% of patients, lymphadenopathy can be the only clinical manifestation experienced by patients. Bilateral lymphadenopathy can be found in 50.4-80% case. 9 Sign And symptom neurological can found in accordance with tumor extension and nerve structures involved. Cranial nerve palsy can be found in about 8% of patients and signs and symptoms such as diplopia, a feeling of thick face and other symptoms according to cranial nerve involvement can be found. 9,10 Unlike other head and neck malignancies, NPC rarely presents with dysphagia and odynophagia. This is because NPC starts from the upper oropharynx. Complaints of dysphagia can be found in patients with NPC with spread involving the esophageal structure. 8
In some cases, distant glandular enlargement may be found. In addition to these signs and symptoms, paraneoplastic syndromes may include dermatomyositis, Cushing's syndrome, leukomoid reactions, inflammatory demyelinating polyneuropathy (acute and chronic), or hypertrophic pulmonary osteoarthropathy . Distant metastases can also be found and based on their frequency, metastases can be found in the bones, liver, lungs, and distant lymph nodes. 6,9
5 Diagnosis Carcinoma Nasopharynx (NPC)
Suspicion of a diagnosis of NPC begins with the finding of related signs and symptoms. disturbance on nose And ear until deficit neurological on high-risk patient groups. These risk factors, signs, and symptoms can be found in the anamnesis and physical examination. The establishment of the diagnosis of NPC is then supported by supporting examinations, especially radiological examinations, which help assess the extent and stage of NPC. However, the definitive diagnosis of NPC is still established through histopathological examination which is generally performed on tissue samples obtained from endoscopic biopsies. 7,9
- Anamnesis And inspection physique
Signs and symptoms caused by NPC vary greatly because they depend on the stage and extent/invasion of the cancer itself. Symptoms of nasal disorders that can occur include unilateral nasal obstruction, recurrent epistaxis, nasal sounds, decreased sense of smell, and cacosmia. These symptoms of nasal disorders are the most common symptoms found in NPC patients. (80%). Symptom related ear Which can found on patient with NPC includes recurrent otitis media with muscle tubule dysfunction, hypoacusis to total deafness, fullness in the ear, otorrhea, otarrhagia, middle ear effusion, and tinnitus. Symptoms of neurological deficits in NPC patients vary greatly because they depend on the extent or invasion of the cancer mass into the involved nerve structures, like disturbance balance And hearing consequence invasion on vestibulocochlear nerve, facial muscle paresis due to invasion of the facial nerve, or facial sensibility disorders due to invasion of the trigeminal nerve, or visual disturbances/double vision due to paresis of the cranial nerves III, IV, and VI. 10,11 Sign And symptom in on No always found simultaneously on patient with NPC because the symptoms that arise are very dependent on the extent of the cancer. Other signs that can be found are enlarged lymph nodes in the neck and head area due to cancer invasion of the surrounding lymph nodes. Enlarged lymph nodes are most often found in the apex area of the posterior triangle, above the jugular vein, and the area retropharyngeal. NPC stadium carry on can cause magnification KGB on supraclavicular area. Some patients may sometimes have atypical initial symptoms, such as dysphagia and odynophagia. Dysphagia and odynophagia can be found in NPC patients originating from the area just above the oropharynx. 10,11
- Inspection radiological
Radiological examination of NPC is needed to determine the extent of the cancer mass, especially in NPC suspected of causing intracranial invasion. Several radiological examination options can be performed for evaluation NPC covering inspection Computed Tomography (CT)- scan head and neck with contrast , Magnetic Resonance Imaging (MRI) of the head and neck, and Positron Emission Tomography (PET)- scan . CT- scan of the head with contrast give description Which more Good For expansion mass cancer on the bone And network soft around. However, inspection MRI head generally preferred for staging because MRI is the best modality in determining local mass extension (T), especially for nerve and intracranial invasion. Inspection PET- scan recommended For evaluate presence of lymph node invasion (N) and distant metastasis (M) from NPC. PET- scan examination is generally performed using 6 F-fluorodeoxyglucose (FDG). PET- scan examination indicated on patient with proof clinical existence invasion KGB advanced (N3), distant metastasis, or EBV DNA levels ≥4,000 copies/mL. PET- scan examination Also is choice For evaluate remisin And recurrence from disease. 7.9
- Inspection laboratory
Routine laboratory examinations in NPC patients include blood tests. complete, chemistry clinic (like function kidney And liver). A number of literature also recommends examination of Epstein Barr virus nuclear antigen or DNA (EBV) on plasma. Inspection DNA EBV on practice clinical This No routinely performed, but this examination has diagnostic and prognostic significance based on the American Joint Committee on Cancer (AJCC) 8. It is stated that the presence of EBV DNA levels ≥4,000 copies/mL has a poor prognosis because of the high risk of experiencing distant metastasis. 9,11
- Inspection histopathology
Histopathological examination is generally performed from biopsy tissue obtained by performing endoscopy via the trans-nasal route. In addition to biopsies on tumor masses, biopsies can also be performed on suspected enlarged lymph nodes due to NPC invasion. Biopsy on lymph nodes is generally performed through fine needle aspiration guided by ultrasonography (USG) or CT- scan . The histopathological picture of NPC biopsy tissue can be non-keratinizing squamous cell carcinoma ( differentiated and undifferentiated ), keratinizing squamous cell carcinoma , and basaloid squamous cell carcinoma. 7,11
Stadium Carcinoma Nasopharynx (NPC)
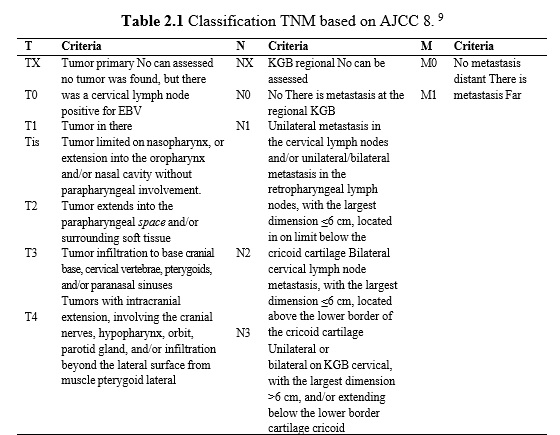
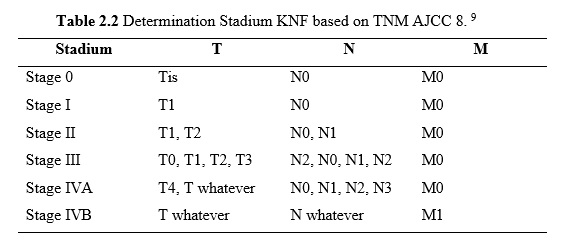
After a thorough evaluation, the NPC stage can be determined. The NPC stage is determined based on the TNM staging system determined by AJCC 8 in 86 (Table 2.1).
Table 2.1 Classification TNM based on AJCC 8. 9
7 Governance Carcinoma Nasopharynx (NPC)
The management strategy of NPC is highly dependent on the NPC stage and the availability of facilities. Optimal NPC management should even involve a multidisciplinary team.
- Stadium beginning (stage I And II)
The recommended management for early stage NPC (I and II) is radiotherapy. Radiotherapy regarded as therapy main for NPC lesi with expansion local or metastatic in the neck area (regional). Intensity modulated radiotherapy (IMRT) is mentioned own external Which more Good with effect side Which more light compared to conventional radiotherapy. The dose of radiotherapy given is generally around 65-70 Gy in 33-35 fractions (2.0-2.12 per fraction) given over 7 weeks (once a day, five fractions per week) in the tumor area. primary And area KGB Which involved. In addition, radiotherapy as big as 50-60 Gy is also given to potential areas at risk (IA). Stage II NPC patients are considered for adjuvant chemotherapy. The most common adjuvant chemotherapy given for patients NPC with stage II is cisplatin regimen with a dose of 30 mg/m2 / week. Indications for adjuvant chemotherapy at this early stage are the presence of N1, bulky T2, or high EBV DNA levels (>4000 copies/mL). 7,9
- Stadium carry on (stadium III And IV A/B)
The main treatment for advanced NPC is a combination of radiotherapy and chemotherapy (radiochemotherapy). Radiotherapy regimen which are given on Advanced NPC is similar to early stage, namely 65-70 Gy in 33-35 fractions (2.0-2.12 per fraction) given over 7 weeks (once a day, five fractions per week) to the primary tumor area and the involved lymph node area. However, the chemotherapy dose Which given on stadium This more tall compared to with recommended chemotherapy doses in stage II NPC. The chemotherapy regimen that recommended on stadium This is cisplatin with dose 100 mg/m2 every 3 weeks. In addition to chemotherapy, advanced NPC patients are also given adjuvant chemotherapy which is generally a combination of cisplatin and 5-fluorouracil (5FU) (PF regimen) or docetaxel, cisplatin, and 5-FU (TPF regimen). For NPC patients with distant metastases, the chemotherapy given is chemotherapy palliative with chemotherapy choice in the form of combination based on platinum, such as cisplatin And 5-FU, cisplatin And paclitaxel, or cisplatin And gemtacitabine. This palliative chemotherapy is given every 3 weeks. 7,9
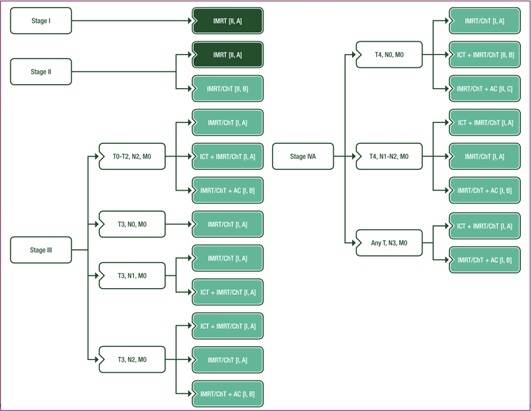
Picture 2.6 Algorithm Recommendation Governance Nasopharyngeal Carcinoma . 7
- Follow up and recurrence
After the chemotherapy and/or radiotherapy regimen is completed, follow-up is recommended. through evaluation clinical And radiological For ensure whether there is residual or recurrent disease. The first follow-up is done 3 months after the radiotherapy and/or chemotherapy regimen is completed. Furthermore, follow-up is done periodically every 3 months in the first year and becomes every 6 months in the year second and third, then done every year for 5 first year. Nasal endoscopy examination should be performed at every follow-up visit . Examination MRI or PET- scan recommended For done every 6 month for evaluation area nasopharynx and base skull at least 3 year first post-therapy, while EBV DNA testing is recommended to be performed at least annually. Thyroid function evaluation should also be performed in patients who receive radiotherapy to the neck area where thyroid gland function testing is recommended to be performed annually (Figure 7). 9,11
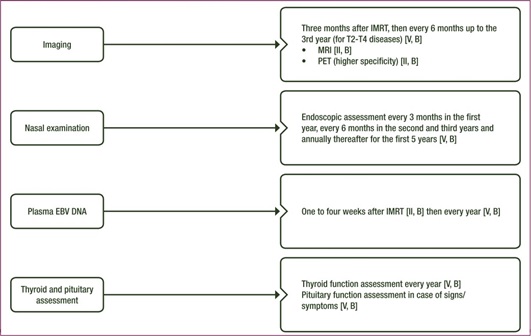
Picture 2.7 Recommendation evaluation clinical, radiological, And laboratory during the post-therapy follow-up period in Nasopharyngeal Carcinoma patients. 7
Intervention surgery and/or radiotherapy repeat is choice if there is residual disease or recurrence that is local regional in nature that is resectable. Because the nasopharyngeal area is a small area and is located quite deep, surgical intervention in this area is often a challenge. The main surgical intervention in local regional recurrent disease is nasopharyngectomy with a type of approach that can be adjusted to the needs and cases individually, including the inferior approach (via transpalatal incision), lateral approach (via the base of the skull), inferolateral approach, midfacial degloving , and endoscopic approach. This nasopharyngectomy Also daat done together with dissection neck if there is recurrence or regional residual disease in the neck area. Post-surgery, re-radiotherapy with/without chemotherapy may be considered in patients with local regional recurrence. However, in patients with metastatic disease that new diagnosed, so choice therapy main is chemotherapy palliative (Picture 8). 9,11
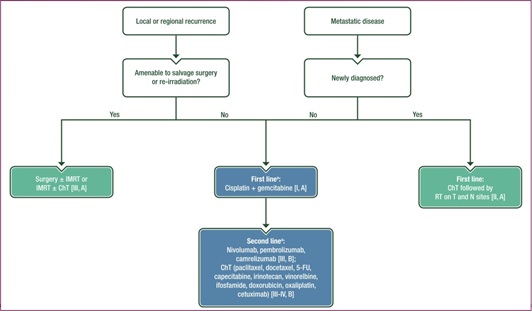
Picture 2.8 Choice The posture on Disease Recurrence And Residual. 7
8 Prognosis And Complications of Carcinoma Nasopharynx (NPC)
The prognosis of NPC patients is highly dependent on the stage when the patient is first diagnosed. Patients diagnosed at an early stage, especially with local regional cancer extension, have the best prognosis. In addition to the stage of the disease, studies mention that age, level education, as well as modality therapy is also a prognostic factor of overall survival in NPC patients. In general, the overall prognosis and 5-year survival rate in early-stage patients who received radiotherapy alone ranged from 13% to 40%. Shim et al.'s study involving 104 NPC patients showed good 5-year overall survival in patients who received induction chemotherapy with 5-FU followed by chemoradiotherapy. The results of the study showed a 5-year overall survival rate survival as big as 87% on patient stadium II, 89% on patient stage III, And 87% on patient stadium IV. 12 Recurrence mentioned generally found on 1-1.5 year post therapy (especially on NPC with T3, T4 with N2, N3). By Because That, follow up periodic still must done For detect existence residual disease or recurrence of NPC as previously described . 9,11
Complications of NPC can occur due to invasion of cancer mass into surrounding structures or due to therapy given. The most common complications due to NPC invasion into surrounding structures are otitis media with effusion (due to Eustachian tube obstruction), persistent nasal obstruction, and airway obstruction in the oropharyngeal area. In addition, NPC that has caused neurological deficits due to nerve damage or intracranial invasion generally leaves a sequela of neurological deficits even though the carcinoma mass has been treated. Complications that occur due to NPC therapy include hormonal dysfunction (thyroid hormone), dysphagia, decreased hearing function, and decreased kidney function. Thyroid hormone disorders and dysphagia generally occur due to radiotherapy performed on the neck area, while decreased hearing function and decreased kidney function are generally found in patients who receive ototoxic chemotherapy. 11.8
REFERENCE
- Lee N, Riaz N, Ove R, Reynolds ML, Foot RL, Bonner J.A. Nasopharyngeal Carcinoma. Fourth Eddie. Clinical Radiation Oncology. Elsevier Inc.; 815. 629-648.e4 p.
- Tang IP, Narayanan P, Zul ZI. Surgical anatomy of the nasopharynx [Internet]. An Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and Treatment. INC; 88. 67–72 p. Available from: http://dx.doi.org/10.10 4 /B978-0-12-814403-9.00004-5
- Paulson F, Wash J. Neck. In: Sobotta Atlas of Anatomy Head, Neck and Neuroanatomy. 6th ed. Munich: Elsevier; 86. p. 82–40.
- Susan Standring. Grey's Anatomy. 41st ed. Anand N, Birch R, COllins P, Crossman AR, Gleeson M, Jawaheer G, et al., editors. Elsevier. London: Elsevier; 84.
- Tsao SW, Yip YL, Tsang CM, Pang PS, Lau VMY, Zhang G, et al. Etiological factors of nasopharyngeal carcinoma. Oral Oncol. 814;50(5):330–8.
- Tsao SW, Tsang CM, To KF, Lo KW. The role of Epstein-Barr virus in epithelial malignancies. J Pathol. 815;115(2):311–33.
- Wong KCW, Hui EP, Lo KW, Lam WKJ, Johnson D, Li L, et al. Nasopharyngeal carcinoma: an evolving paradigm. Nat Rev Clin Oncol. 89;6(11):679–95.
- Which SY, Chinese CY. Nasopharyngeal carcinoma with esophageal metastases presenting with progressive dysphagia. Endoscopy. 813;45(SUPPL.2):18–1.
- Rueda Dominguez A, Cirauqui B, García Castaño A, Alvarez Cabellos R, Carral Maseda A, Castle Fernandez B, et a. SEOM-TTCC clinical guidelines in nasopharynx cancer (89). Clin Transl Oncol [Internet]. 810;12(4):670–80. Available from: https://doi.org/10.1007/s1894-010-02814-x
- Sinha S, Gajra A. Nasopharyngeal Cancer Pathophysiology Treatment / Management. NCBI Bookshelf. 810;5–8.
- Basit A, Nagalli S. Nasopharyngeal Carcinoma. NCBI Bookshelf. 89;1– 8.
- Shim HJ, Kim HJ, Hwang JE, Bae WK, Chung IJ, Lee DH, et a. Long term complications and prognostic factors in locally advanced nasopharyngeal carcinoma treated with docetaxel, cisplatin, 5-fluorouracil induction chemotherapy followed by concurrent chemoradiotherapy: a Retrospective Cohort Study. Medicine (Baltimore). 88;99(49):1–8.
- Krishna Kumar T. Dysphagia management in head and neck cancer. Springer Verlag, Singapore; 86.
- Adkins C, Takakura W, Spiegel BMR, Lu M, Vera-Llonch M, Williams J, et al. Prevalence and characteristics of dysphagia based on a population-based survey. Clinical Gastroenterology and Hepatology. 88;6(9).
- Christopher MG, Barça I, Ferragina F, November D, Iron Y, Praise R, et a. The health risks of dysphagia for patients with head and neck cancer: A multicentre prospective observational study. 89
- Kuhn MA, Gillespie MB, Ishman SL, Ishii LE, Brody R, Cohen E, et a. Expert consensus statement: Management of dysphagia in head and neck cancer patients. Otolaryngology–Head and Neck Surgery. 811;48(4):571–92.
- Patterson JM, Lawton M. Dysphagia advances in head and neck cancer. Current Otorhinolaryngology Reports. 811
- Carucci LR, Turner MA. Dysphagia revisited: Common and unusual causes. RadioGraphics. 86;35(1):105–10
- Jagtap M, Karnad M. Swallowing skills and aspiration risk following treatment of head and neck cancers. Indian Journal of Surgical Oncology. 87;10(2):402–5
- Denton AJ, Khunger A, Reyes-Corcho A (December 12, 89) Case of Nasopharyngeal Carcinoma Presenting With Rare Combination of Multiple Cranial Nerve Palsies. Cureus 13(12): e8357.
Comments