Orbital Floor Fractures
I Made Nudi Arthana
Orbital Floor Fractures is fracture on base orbit Which is structure most thin on the orbital wall 1 . The orbital floor is the most common location of orbital fractures, accounting for 47.9% from all fracture orbit, followed by fracture wall medial (25%), wall lateral, and the roof of the orbit. The most common occurrence is in young adults. Orbital fractures most commonly caused by blunt trauma to the midface 2,3 .
LITERATUR REVIEW
Anatomy Orbit
The orbits are a pair of bony cavities shaped like quadringular pyramids. The orbits are bounded by a roof, a floor, and medial and lateral walls. The base of the orbits is located in anterior, to form aperture orbital, And the apex located in posterior And ends at the optic foramen. The medial wall is separated by the ethmoidal sinus at an average distance 25 mm And almost parallel. Wall medial And lateral orbit to form corner around 45 ° . One-fifth of the orbital volume is filled by the eyeball. In addition, the orbit is also filled by extraocular muscles, blood vessels, nerves, nasolacrimal apparatus, connective tissue, and fat tissue 11,12 .
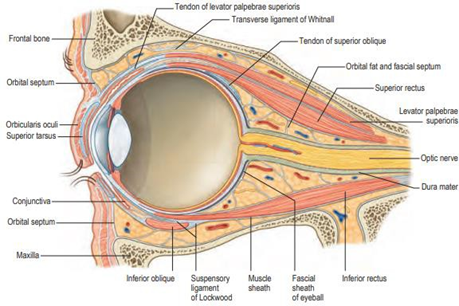
Picture 1. Orbit And Structure Anatomical in Inside 12
Wall orbit formed by 7 bone, that is OS frontal, zygoma, maxilla, lacrimal, ethmoid, palatine, and sphenoid. The roof of the orbit is formed by the orbital part of the frontal bone anteriorly which separates it from the orbit with fossa cranial anterior, And style minor OS sphenoid in posteromedial. On the anterolateral side of the roof of the orbit, there is a lacrimal fossa which houses the lacrimal gland. Whereas on side anteromedial there is fossa/fovea trochlear, Which become attachment site of trochlear apparatus 11,12,13 .
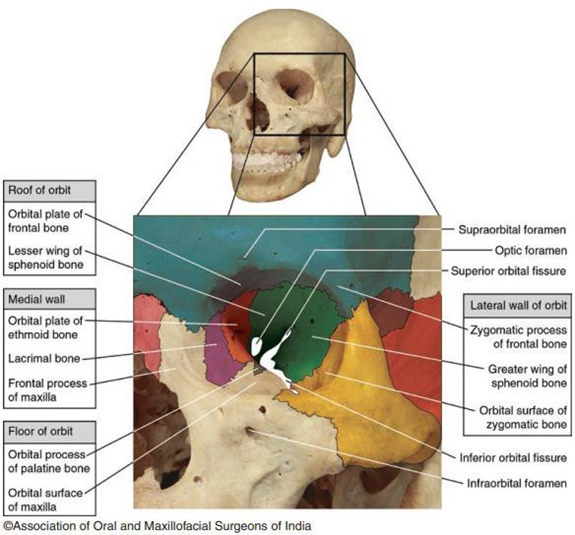
Picture 2. Anatomy Orbit 14
The lateral wall of the orbit is the thickest and strongest wall of the orbit, consisting of the frontal process of the zygoma bone anteriorly and the major ala of the sphenoid bone posteriorly, which are fused together. on suture sphenozigomatics. Wall lateral orbit most thick on part posteriorly, where it separates the orbit from the middle cranial fossa. The greater and lesser ala of the sphenoid bone are separated by fissure orbitalis superior. There is two structure on wall lateral orbit, namely the lacrimal foramen through which the recurrent meningeal artery passes and the zygomatico-orbital foramen through which the zygomaticofacial and zygomaticotemporal nerves pass.12,13
Pars orbitalis OS ethmoid (lamina papyracea), pars orbitalis OS frontalis, corpus OS The sphenoid, lacrimal bone, and frontal process of the maxillary bone form the medial wall of the orbit. The lamina papyracea is very thin with a thickness of about 0.2-0.4 mm. There are several structures on the wall medial orbit, between other sulcus lacrimal Which occupied by pocket lacrimal, and the anterior and posterior ethmoidal foramen through which the ethmoidal blood vessels and nerves pass. Trauma to the medial wall of the orbit can cause epiphora, massive epistaxis, and damage to the rectus medius muscle 1,12,13 .
The base of the orbit is formed from 3 bones, namely the pars orbita of the maxillary bone, the zygoma bone in the anterolateral part, and the processus orbitalis OS palatine on the posteromedial side. The orbital floor is thin and at the same time become limit on from sine maxillary. Base orbit is part Which weakest of the orbital structures. There are three important structures at the base of the orbit, namely the rectus muscles inferior, nerve infraorbital, And vessels blood infraorbital. Nerve infraorbital pass foramen intraorbital, give innervation sensory on area Which located ipsilateral to base orbit as well as part middle face, that is on petals eye lower, part edge nose, septum nasal, part front cheek, And part lips on. This foramen Also passed by by infraorbital artery which is a branch of the maxillary artery 1 .
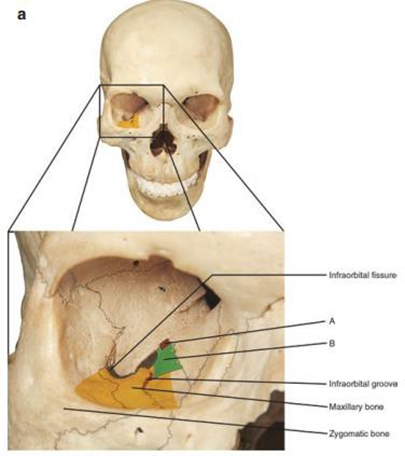
Picture 3. Structure Base Orbit 14
Apex orbit located in posteromedial, formed by corpus, style major, And style minor sphenoid bone. This structure is very complex. The optic canal at the apex of the orbit is traversed by the optic nerve and its meningeal sheath, as well as the ophthalmic artery. The tendinous annulus (annulus of Zin) which is origin from four muscular rectus, attached in near canal This, specifically at its superior, inferior, and medial borders. The superior orbital fissure is the gap between the greater and lesser ala of the sphenoid bone, through which the oculomotor, trochlear, and abducens nerves pass (1,12,13 ).
Orbital Floor Fractures
Definition
Orbital floor fracture is a fracture that occurs at the base of the orbit which is the thinnest structure on the orbital wall 1 . In orbital fractures, the term blowout fracture is known, which is a condition where the fracture fragment shifts away from the orbit. While blow-in fracture is a condition where the fracture fragment shifts into the orbit 15 .
Epidemiology
Orbital fractures may occur in association with other maxillofacial fractures and often involve multiple orbital wall fractures 2 . Orbital fractures are found in 30-55% of all facial region fractures 16 . The orbital floor is the most common location of orbital fractures, accounting for 47.9% from all fracture orbit, followed by fractures of the medial wall (25%), lateral wall, And roof orbit. Incident most obtained on person mature young, especially in the first 3 decades of life 2.3 .
Incident on man Far more Lots compared to on woman, that is reach 85% 17 . On injury sport, 21% among them is trauma maxillofacial, And 17% among them experienced orbital floor fractures 7 . Orbital floor fractures generally occur unilaterally, while bilateral fractures only occur in 5% of cases 8 .
Etiopathogenesis
Orbital fracture most often caused by blunt trauma to the middle part of the face, such as in traffic accidents, sports trauma, abuse, work accidents, or falls 2,8,17 . Orbital fractures can occur alone or in conjunction with other fractures in adjacent bones, such as naso-orbital-ethmoidal fractures, zygomaticomaxillary complex fractures, or Le Fort II/III 18 .
There is 2 mechanism Which underlying the occurrence Orbital Floor Fractures, that is the transfer of kinetic energy from the bones around the orbit causing the floor of the orbit to bend and fracture (theory buckling ), or improvement pressure ball eye consequence compression structure orbit which causes pressure on the orbital wall until a fracture occurs (hydraulic theory) 1,17,18 .

Picture 4. Biomechanism The occurrence Orbital Floor Fractures 14
Orbital floor fractures can cause distortion of the volume and shape of the orbit, resulting in visual or cosmetic impairment 4 . There are 3 anatomical structures that can be injured by orbital floor fractures, that is muscular rectus inferior, nerve infraorbital, and infraorbital vessels 1 .
The inferior rectus muscle is located just above the floor of the orbit and can be injured if fragment bone from wall orbit shift to superior. Injury muscle Which experienced can be contusion, transsection, damage total, tear longitudinal. Appropriate in on muscular The inferior rectus is the inferior branch of the oculomotor nerve, which may also be damaged depending on the severity of the injury. Muscle injury with or without oculomotor nerve injury can cause diplopia and inability of the eye to infraduce 1 .
Orbital floor fractures can also cause damage to the infraorbital nerve. This nerve passes through the infraorbital foramen and lies inferior to the orbital floor. It supplies sensory innervation to the orbital floor, midface, skin of the inferior eyelid, nasal margin, nasal septum, anterior cheek, and upper lip. Damage to this nerve can cause hypoesthesia, dysesthesia, or hyperalgesia on the affected side 1 .
Infraorbital artery injuries generally occur in more complex orbital fractures and are rare in pure blowout fractures , but can cause massive bleeding because it is a branch of the maxillary artery 1 .
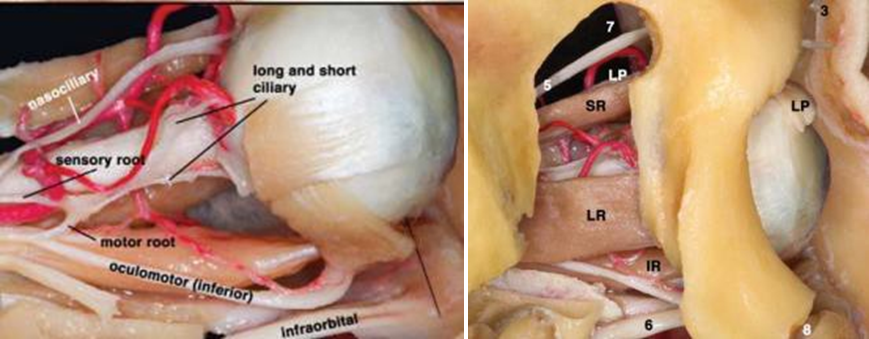
Picture 5. Structure Anatomy Which Can Experience Injury On Fracture Orbital Base. IR: inferior rectus muscle; 6: infraorbital nerve 13
On generally, fracture orbit is fracture open door , that is fracture comminuted which is accompanied by with shift fragment fracture. If fracture happen in a way linear followed with prolapse network soft orbit (muscular rectus inferior or fat periorbital inferior) to maxillary sinus, then the fracture fragment shifts back to its original position so that the orbital tissue or extraocular muscles are trapped in between the fracture fragments, this condition is called a trap door fracture 19 . Fracture trap door Which Also known as fracture white eyes or green stick generally occurs in children due to high bone elasticity, and is often only found in pure/isolated orbital floor fractures 1,8,19,20 .
Symptom Clinical and Diagnosis
In patients with trauma to the maxillofacial region, first an evaluation of the airway, breathing, and circulation should be performed according to the ATLS protocol 21. Next, anamnesis should be performed. And inspection physique comprehensive, followed with inspection on region trauma 18 .
Anamnesis
Anamnesis should include the mechanism of trauma and the symptoms experienced 7 . The mechanism of trauma should covers size the thing that cause trauma and energy or speed of the object 8 . Symptoms of orbital floor fractures include diplopia especially when moving the eyeballs, visual disturbances, infraorbital nerve dysfunction which is clinically characterized by hypoesthesia, dysesthesia, or hyperalgesia on the affected side, eye pain, and nausea and vomiting which are aggravated by moving the eyeballs. Nausea and vomiting can occur due to vagal reflexes caused by increased intraorbital pressure due to trapped orbital soft tissue. In addition to nausea and vomiting, syncope can also occur. This is called the oculocardiac reflex 1,3,8 .
Inspection Physique
The physical examination begins with checking vital signs and a complete physical examination, followed with inspection ophthalmologist 7 . Wrong One Which need be aware namely bradycardia, arrhythmia, or heart block which can be caused by the oculocardiac reflex 3. Evaluation on region trauma between other evaluation periorbital, evaluation ball eye, motion ball eyes, vision, and intraocular pressure examination 8 .
In the evaluation of the periorbita and orbit, periorbital edema, periorbital ecchymosis (75%), subconjunctival hemorrhage (40%), open wounds, hypoglobus, enophthalmos (33%) can be found. chemosis conjunctiva, hyphema, And limited motion ball eye. Enophthalmos is shifting of the eyeball posteriorly on the anteroposterior axis, while hypoglobus is the shifting of the eye to the inferior due to the loss of the integrity of the basic structure of the eyeball. Enophthalmos examination can be done with an exophthalmometer. In shifts of more than 2 mm, enophthalmos can detected in a way clinical 8.19 . Palpation rhyme orbit in inferior part step-off deformity and tenderness may be present 8,18 .
In cases of trap door fractures , there is generally no significant injury to the periorbital soft tissue so that clinically the orbital region may appear calm and the clinical symptoms that appear are generally limited eyeball movement when trying to supraduce and diplopia. However, this type of fracture is often associated with the occurrence of oculocardiac reflexes 19,20 .
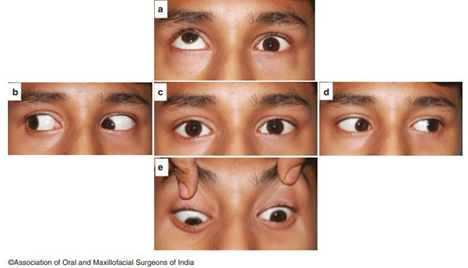
Picture 6. Limited motion ball eye to superior And inerior on fracture left orbital base 14
Inspection Support
Computed tomography ( CT) scan without contrast is the standard examination. gold on case fracture orbit 7.17 . Through inspection CT scan, can evaluated location and wide fracture as well as injury on network soft orbit. Piece < 2 mm with 3D reconstruction can provide optimal evaluation of the orbital bones. Coronal and sagittal sections can help identify fractures in the orbital floor, while axial sections are more helpful for evaluating medial orbital wall fractures. Entrapped soft tissue, hematoma retrobulbar, emphysema, or stretch it nerve optician can evaluated in soft tissue setting. CT scan is also very helpful in planning operative action 22 . In cases of trap door fractures , a typical sign called the tear drop sign can be found, namely the image of orbital tissue entering the maxillary sinus 19 .


MRI is generally not is required in diagnosing orbital trauma. However, MRI may be considered to help determine further management strategies in difficult cases, for example if intraorbital soft tissue injury or optic nerve, extraocular muscle, or cavernous sinus injury is suspected 7 .
Management
Management of orbital floor fractures can be divided into conservative therapy and surgical intervention 7 .
Therapy Conservative
Most cases of orbital fractures can be treated conservatively. Some indications for therapy conservative that is patient with diplopia minimum, motion ball eye Which Good, And there is no significant enophthalmos or hypoglobus 6 . Cold compresses and head elevation are recommended to help reduce periorbital edema. Prophylactic steroids and antibiotics can be considered in cases of severe periorbital edema, to prevent orbital cellulitis. However, antibiotic administration still requires further research. All patients with orbital floor fractures are educated not to blow air/secretions forcefully from the nose, because it can trigger orbital emphysema and orbital compartment syndrome 2 .
Surgery
Surgical therapy aims to restore compressed tissue, reposition ball eye, close defect bone, And return volume orbit so that repair function ocular 23 . Indication from surgery on case Orbital Floor Fracturesa soon to moment This still many researched, However a number of indication absolute Which mentioned in the literature, namely limited eye movement with signs of muscle compression both clinically and radiological, reflex oculocardiac persistent, And enophthalmos 2 mm or more. Meanwhile, relative indications for surgical procedures include persistent diplopia for more than 7-10 days when the eye position is neutral and the defect area is more than 50% or with an area of 1.5-2 cm2 or more 14,6,23 .
Immediate surgery is an operative procedure performed within 24-48 hours after trauma occurs . 19 Indications for immediate surgery include signs of oculocardiac reflex, enophthalmos, or significant acute hypoglobus that causes asymmetry. face, as well as fracture trap door with sign compression muscle 6 . Most case Orbital fractures do not require immediate surgical treatment, and treatment can be performed 4-14 days after trauma 22,24,25 .
Some literature states that if there is no indication for immediate surgery, surgery should be performed after the ecchymosis and periorbital edema have decreased. This also aims to provide more time to prepare for surgery and implants that will be used if needed 2,22 . However, delaying the procedure also has disadvantages, including adhesions and the formation of fibrotic tissue around the tissue. soft orbit that can complicates action and affect the recovery of eye movement and vision 25 . Thus, if surgery is required, it should be performed no later than 14 days after the trauma 6 .
Some relative contraindications for surgical procedures are if there is a retinal tear, hyphema, lens dislocation, eyeball rupture, or avulsion trauma to the eyeball that requires more immediate treatment than fracture reconstruction, as well as conditions where the patient can only see with one eye (monocular) and fracture reconstruction is at risk of causing decreased vision in the eye that can see 6,14 .
Some surgical techniques that can be chosen are the subciliary, subtarsal, transconjunctival approaches. as well as endonasal or transantral with endoscopy 7,8,9 . Control post surgery was scheduled on the first day, first week, first month, third month, and sixth month, and first year. After surgery, success criteria included enophthalmos < 2 mm, as well as improvement in ocular motility disorders, diplopia, and strabismus 24 .
Approach subciliary And subtarsal
In the subciliary and subtarsal approaches, local anesthesia with epinephrine is infiltrated intravenously. subcutaneous on petals eye lower And throughout edge orbital inferior. Lateral tarsorrhaphy
temporary is performed on the operative side for protection and retraction. A subciliary skin incision is made 2 mm below and parallel to the lash line using a no. 15 blade. The incision should not be made more medial than the lower lid punctum. Laterally, the incision can be extended up to 15 mm beyond the lateral canthus 21 .
Dissection is performed sharply inferiorly or using a Colorado dissector, until reaching the tarsal plate in a plane superficial to the orbicularis oculi muscle to maintain the inferior eyelid structure. The dissection process is then continued toward the orbital rim in the preseptal plane until reaching the periosteum. The periosteum is incised anteriorly to the inferior orbital rim, and elevation is continued posteriorly to the orbital floor using a periosteal elevator 7,21 .
Approach subtarsal is variation from approach subciliary. Incision skin made in the subtarsal fold or 5-7 mm from palpebral margin inferior if the fold can not seen due to edema. The incision begins at the level of the inferior lacrimal punctum to the lateral border of the orbital fissure. The muscle orbicularis eye separated from skin, after That incised until looks anterior surface of the tarsoorbital fascia. Dissection is continued in the preseptal plane, following the orbital septum until reaching the infraorbital rima 7,8 .
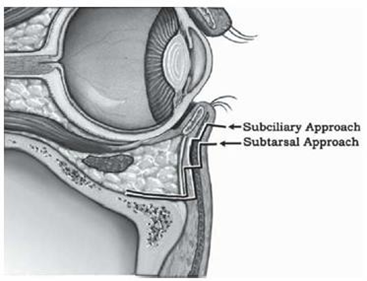
Picture 8. Approach Subciliary And Subtarsal 7
Approach transconjunctival
The transconjunctival approach is gaining popularity when compared to the transcutaneous approach. Because lower risk the occurrence malposition palpebra inferior 7 . For preparation approach transconjunctival, anesthesia local with epinephrine infiltrated in canthus laterally, just beneath the lower lid conjunctiva, and transcutaneously to the orbital rim. Lateral canthotomy and inferior cantholysis can be performed using iris scissors to improve visualization roomy operation And minimize retraction petals lower. If release cantus No done, must very be careful For avoid excessive retraction which can cause malposition of the inferior palpebra 21 .
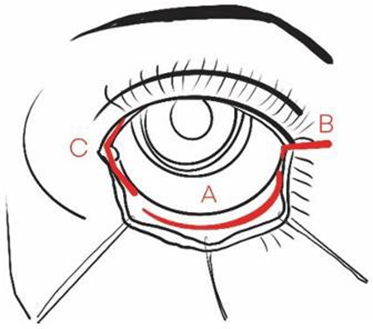
Picture 9. A) Approach transconjunctival; B) Extensions to lateral (canthotomy/cantholysis); C) Extension into the media (transcaruncular) 22
The incision is made from the medial to lateral or lateral to medial side through the conjunctiva, 1 mm below the inferior margin of the tarsal plate. Preseptal dissection to separate the orbicularis muscle eye And septum done in a way blunt direction edge orbital inferior. After The inferior orbital rim is visualized, subperiosteal dissection is performed posteriorly. This dissection can be extended up to 25 mm posteriorly from the inferior and lateral rim. Important structures such as the infraorbital nerve, inferior oblique muscle, lacrimal apparatus, and optic nerve must be spared during surgery 9 .
After that, the periosteum was elevated from the orbital floor using a Freer periosteal elevator. After the fracture site was identified, soft tissue trapped in the fracture fragments was released and implants were placed. The wound was then closed and sutured 24 .

Picture 10. Approach transconjunctival. a) Incision transconjunctival made below the inferior border of the tarsus, dissection is performed between the orbicularis muscle and the septum
orbit. b) Network soft Which have a herniation released from area fracture. c) And
d) installation implant subperiosteal For close defect 24
Approach Endoscopic
The transantral endoscopic approach to the orbital floor can be used alone or in combination with a more traditional periorbital approach to aid in visualization and reduction of the fracture. The technique begins with an incision in the gingivolabial sulcus. The maxillary periosteum is then incised. The lips are retracted, and a periosteal elevator is used to expose the anterior wall of the maxillary sinus. A Kerrison osteotome and rongeur are used to create the defect. measuring 10 x 20 mm on the anterior wall of the maxillary sinus. A mucosal layer measuring 4 to 5 mm on the gingival side must be maintained to close the defect 8,21 .
Telescope 4 mm with corner 0 And 30 degrees Then entered through antrostomy to visualize the orbital floor. The defect in the floor is usually clearly visible, and the mucosa can be elevated in around defect For help visualization And reduction Contents orbital. Fracture Trap door or greenstick type fractures can sometimes be reduced using this approach alone without the need for fixation if the fracture fragments are back in place. Implants can also be inserted if necessary by first placing them posteriorly and then sliding them anteriorly 21 .
Closure is accomplished by reattaching the gingivolabial sulcus mucosa. Reported advantages of the transantral approach include better visibility of the orbit posterior And especially on part posterior from defect. The drawbacks covering difficulty in reconstructing the orbital floor located lateral to the infraorbital nerve and the need for special endoscopic instruments 21 .
In addition to the transantral approach, another technique that can be chosen is the endonasal endoscopic approach. Some techniques that have been used include through the middle meatal antrostomy or the prelacrimal approach 26,27 . In the prelacrimal approach, the maxillary sinus antrum is accessed through the prelacrimal recess, which is a depression in the anterosuperior part. side medial wall sine maxillary, Which located in between duct nasolacrimal and piriform aperture 28 .
The prelacrimal approach begins with the administration of topical decongestants. After that, uncinectomy And middle meatal antrostomy. Incision curved done with a sickle knife in line with the maxillary line, at the level of the piriform aperture and extended inferiorly to the floor of the nasal cavity. Subperiosteal dissection of the lateral nasal wall and inferior meatus is then performed. A vertical osteotomy is performed posterior to the mucosal incision at the level of the inferior concha attachment, between the piriform aperture and the axillary inferior concha. This osteotomy is performed with a chisel or a high-speed drill with a diamond burr , depending on the thickness of the frontal process of the maxillary bone. The medial wall of the sinus together with duct nasolacrimal Then medialized. After That, wall The medial maxilla and inferior concha are returned to their original positions 28 .

Picture 11. Reconstruction Orbital Floor Fractures with Approach Transantral and Prelacrimal Endoscopy 27,29
Use Implant on Orbital Floor Fractures
Orbital floor fractures are different from other maxillofacial fractures in general, where the fragments Orbital Floor Fractures resemble fraction shell egg. Implant Which ideal should be enough thin, light, strong withhold burden, flexible, resistant to infection, non carcinogenic, non-allergenic, and compatible for MRI machines. Various implant variations have been used in orbital floor fracture reconstruction, such as autograft, allograft, and alloplastic materials 2,16,30 . Some indications for choosing implants in orbital floor fractures can be seen in Table 1.
Table 1. Material Implant And The indication is 30
| Implant Materials | Indication |
Autograft | Bone | Patient pediatrics (< 7year) |
Cartilage | Minor fracture | |
Alloplast | Layer Whichcan be absorbed | Patient pediatrics |
Polyethylene porous | Defect with limits firm | |
Titanium mesh | Defect Which wide,defects small withlimit lateral and stable medial |
Autograft And Allograft
Autograft was previously the gold standard implant choice for orbital floor fracture reconstruction 10,31 . Autologous materials that can be used for orbital fracture cases are bone and cartilage. Bone can be taken from the calvaria, maxilla, ileum, mandible, ribs, tibia, scapula, and sternum. Calvaria bone is a good choice, because it has a large cortical volume so it is more resistant to resorption 31 .
Bone autografts have good strength, can be fixed to the surrounding bone, are radiopaque, and have good biological compatibility. The main disadvantages of using autologous bone tissue in craniofacial reconstruction are the potential for morbidity at the graft site , increased duration and complexity of surgery, varying levels of resorption (up to 86%), difficult to shape due to its rigidity, and bone resorption can cause complications 7,30 .
Autologous cartilage is generally taken from the ear, ribs, and nasal septum 7,30 . Advantages from graft cartilage that is the taking easy, easy formed, Enough strong, and minimal morbidity at the graft site. The disadvantages of cartilage grafts are that they are less strong than bone grafts and are difficult to shape. Cartilage grafts can be considered for small defects 31 .
Alloplastic
Alloplastic grafts do not contain living cells but have osteoinductive/osteoconductive properties 31 . Material alloplastic can differentiated become substrate Which absorbable and non-absorbable. Synthetic alloplasts that can be absorbed include poly-L-lactic acid , polydioxanone, sour polyglycolate, And polymer composite. Type implant This will replaced by fibrous granulation tissue as the body absorbs it 3 . Implants made from polyglycolic acid are generally 95% absorbed after 9 months 31 . The advantages of this type of implant are that it is easy to obtain, easy to shape, and helps facilitate bone growth. However, this type of implant often causes severe inflammatory reactions that cause ocular muscle adhesions, diplopia, enophthalmos, and dystopia 20 . In addition, this type of implant is radiopaque and therefore not visualized on postoperative radiological examination 7 .
Implant alloplastic permanent Which has used For reconstruction base orbit including porous polyethylene, titanium mesh, and silicon. Titanium is a material that is currently widely used because it is biocompatible, anti-rust, rigid, easy to shape, thin, easy to stabilize, can fixate area fracture with Good, And can visualized with both on postoperative CT scans. Porous polyethylene has the advantage of allowing the growth of vascular on area fracture. Lack from implant alloplastic permanent namely, it is a foreign object so it can trigger inflammatory reactions, fibrosis, infection, and can migrate to other locations 3,20,31 .
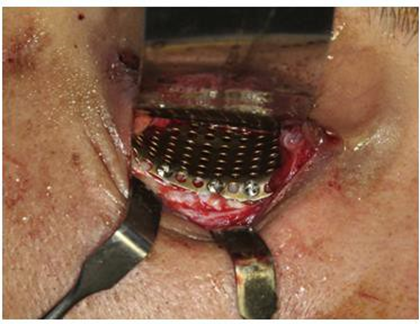
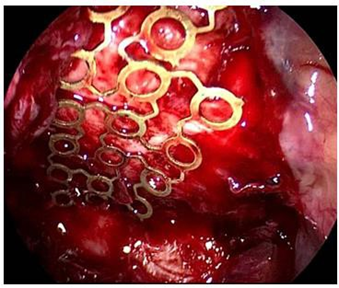
Picture 12. Implants titanium mesh
Complications
Complications of orbital floor fractures can occur due to initial trauma or iatrogenic causes. action surgery. A number of complications Which can happen consequence fracture between other hematoma retrobulbar, emphysema orbit, infection, diplopia persistent, enophthalmos, fistula
sinoorbital, ball dislocation eye to sinus maxillary, as well as neuropathy nerve optic nerve and infraorbital nerve 11 . Failure to diagnose a fracture that requires immediate treatment can result in fibrosis, contracture, and fracture malunion 6 .
Intraoperative complications include injury to the globe and optic nerve caused by direct trauma, excessive retraction, and orbital hemorrhage. Postoperative complications may include visual loss, traumatic optic neuropathy, diplopia, inferior lid retraction, hemorrhage, infection, orbital implant extrusion, infraorbital nerve damage causing hypoesthesia, orbital congestion, and epiphora 6 . Diplopia occurs in 20-50% of patients. Malposition of the inferior lid either ectropion or entropion found in 5% of cases 20 .
DISCUSSION
The right time to perform surgery in cases of orbital floor fractures is still controversial. If there is no indication for immediate surgery, several expert recommend observation for 1-2 Sunday For allow spontaneous reduction of edema and diplopia2,10,20 . On the other hand, delaying operative intervention carries the risk of causing fibrosis And diplopia chronic. So that a number of study state Surgical action should be carried out no later than 2 weeks after the trauma occurs .
Research by Soliman et al. stated that 5.9% of patients with orbital floor fractures required immediate surgery, and 8.8% of patients who received conservative therapy turned out to require surgery during the next check-up. The interval for the emergence of surgical indications in patients who had previously undergone conservative treatment was 5 days after trauma. Therefore, it is recommended to conduct an evaluation 5-10 days after trauma to determine whether surgery is needed 4 .
Approach surgery Which ideal on case Orbital Floor Fractures that is allows visibility And access Which good 16 . Profit approach subciliary And subtarsal is This technique is easy to learn and allows wide access to the orbital floor 21 . The subciliary approach allows clear visualization of the fracture area, making surgery easier. However, the subciliary approach associated with increased visibility used wound and more risk tall the occurrence malposition petals eye consequence cicatrix And ectropion post operation, and other complications 2 .
A meta-analysis compared the incidence of complications between the transconjunctival and subciliary approaches. The transconjunctival approach resulted in a higher complication rate overall Which more low (2.1%) If compared to with approach subciliary (19.1%) and subtarsal (9.7%). The transconjunctival approach is currently preferred by experts because of the risk of scarring. minimal and provides good results and minimizes damage to the infraorbital nerve. However, this approach has a higher degree of difficulty, makes it difficult to visualize the posterior part of the orbital floor, and often requires secondary surgery 2,3 .
Endoscopic surgery through transnasal and transantral approaches has several advantages, including better visualization of the orbital floor, especially in the posterior part, avoiding complications and scars on the eyelids, and avoiding postoperative infraorbital nerve hypesthesia. The endoscopic approach also reduces bleeding during surgery and shortens the patient's hospitalization period, and has high effectiveness in reconstructing orbital floor fractures 2,3 . For surgeons who are accustomed to using endoscopes, this approach is more familiar compared to the transconjunctival or transcutaneous approach 26 .
However, the endoscopic approach has a higher level of difficulty 26 . Besides That, approach endoscopic transantral can cause a number of complications due to antrostomy, like fistula oroantral, edema on face, flavor numb on tooth And gum, recurrent sinusitis, and sensitivity disorders in the superior alveolar nerve area 32 . Kerdoud et al. and Saha et al. suggest a combination of endoscopic techniques and open reduction in more complex fracture cases. The combination of these two techniques has the advantage of good visualization of the entire defects, better soft tissue reduction, and accurate confirmation of graft or implant position 29,33 .
Lee et al.'s research stated that radiographically, bone union is generally visible 4 Sunday after operation. On Sunday 8th, defect bone has united And No there is an area radiolucent Which detected. If patient choose the procedure conservative, recommended to avoid give pressure on area orbit during 4 Sunday And No to expel air/secretions from nose with hard until 12 Sunday after trauma, Because wall the floor and medial orbit are thin and weak 34 .
Implants used for orbital floor reconstruction include autografts and alloplastics. Implant autolog during This considered as gold standard on reconstruction orbital base Because own biocompatibility Which best, However there is risk morbidity at the graft site and have varying degrees of resorption. Alloplastic implants have good strength and can be used in the long term, but are foreign objects that can trigger inflammatory reactions, infections, and the formation of fibrotic tissue. Research Shivam et a. show that implant silicone most often cause occurrence of postoperative complications, namely 17.5%. Followed by polyglactin (14.3%), polyethylene (5.4%), titanium (2.4%), and the least frequent complication is polydioxanone (0.1%) 31 .
CONCLUSION
Diagnosis and management of orbital floor fractures remains a challenge to date because structure anatomy Which complex And height level difficulty action reconstruction. Partly big Orbital Floor Fractures can handled in a way conservative, However failure in diagnosing fractures that require immediate treatment can result in permanent complications. Physical and supporting examinations are very important to determine the indications for surgery. There are several surgical approaches that can be chosen, including subciliary, subtarsal, transconjunctival, transantral, or endonasal. There are several implant options, each of which has certain indications, advantages, and disadvantages.
REFERENCE
Ghosh SK, Narayan RK. Fractures involving bony orbit: A comprehensive review of relevant clinical anatomy. Transl Res Anat. 2021;24:100125.
Pandya RP, Deng W, Hodgson N. Current Guidelines and Opinions in the Management of Orbital Floor Fractures. Otolaryngol Clin N Am. 2023;56:1101–1112.
Patel S, The Shokri T, Zia K, Light Hall J.G. Controversies and Contemporary Management of Orbital Floor Fractures. Craniomaxillofac Trauma Reconstr. 2021;12(4):257–264.
Soliman L, Sawicki N, Sobti N, Swartz S, Rao V, Woo US. Re-evaluating the Timing of Surgery after Isolated Orbital Floor Fracture. Plastic and Reconstructive Surgery – Global Open. 2023;11(5):p.e4973.
Folklore L, Jonsson L, Karlsson T. Orbital floor fractures—a comparison between CT images and findings at surgery. Eur Arch Otorhinolaryngol. 2023; 280:2795–2803.
Dasukil S, Arora G. Indications & Timing Of Orbital Fracture Repair: A Dilemma. Int J Curr Adv Res. 2018;7(5):12894-12897.
Flynn J. Approach to Orbital Fractures After Athletic Injuries. Facial Plastic Heaven Clin N Am. 2022;30:31–45.
Nikolaenko VP, Astakhov YS. Orbital Fractures—A Physician's Manual. Saint-Petersburg: Springer. 2015.
Kim HS, Jeong EC. Orbital Floor Fracture. Arch Craniofacial Surg. 2016;17(3):111- 118.
Pidro A, Jovanovic N, Kadribasic E, Barucija N, Leto N, Kahana A. Delayed Management of an Orbital Floor Blow-out Fracture. Beyoglu Eye J. 2021;6(3):249- 253.
Moore KL, Dalley AF, Agur AMR. Moore Clinically Oriented Anatomy. 8 th Edition. Philadelphia: Wolters Kluwer: 2018.
Standby S, et a. Gray's Anatomy The Anatomical Base Of Clinical Practice 41st ed. Elsevier Limited. 2016.
Love S, Fernandez Miranda JC. Anatomy of the Orbit. J Neurol Heaven B. 2020;81:319- 332.
Bonanza K, Panneerselvam E, Manual S, Kumar VV, Rai A. Oral and Maxillofacial Surgery for the Clinician. Singapore: Springer. 2021.
Valencia RP, Miyazaki H, That M, Nishimura K, Kashizaki H, Tahakashi Y. Radiological findings of orbital blowout fractures: a review. Orbit. 2021;40(2):98-109.
Chattopadhyay C, Dev V, Pilani D, Harsh A. Reconstruction of Orbital Floor Fractures with Titanium Micromesh: Our Experience. J. Maxillofac Oral Surg. 2022;21(2):369- 378.
de Santana IHG, Viana MRM, Palhano-Dias JC, Ferreira-Junior O, Sant'Ana E, Shinohara EH, et al. Orbital floor fracture (blow out) and its repercussions on eye movement: a systematic review. Eur J Med Res. 2024;29:427.
Lazar A, Bhakta P, Arango A, Brookes C. Commentary- Does Early Repair of Orbital Fractures Result in Superior Patient Outcomes? A Systematic Review and Meta-Analysis. J Oral Maxillofac Surg. 2020;78:e11-e14.
Al-Qattan MM, Al-Qattan YM. “Trap Door” Orbital Floor Fractures in Adults: Are They Different from Pediatric Fractures? Plast Reconstr Surg Glob Open. 2021;9(4):e3537.
The Shokri T, Alford M, Hammons M, Ducic Y, Sokoya M. Management of Orbital Floor Fractures. Facial Plast Surg. 2019;35:633–639.
Johnson J & Rosen C, editors. Bailey's Head and Neck Surgery Otolaryngology. 5th Edition. Baltimore: Lippincott Williams and Wilkins: 2014.
Gooris PJJ. Mourits MP. Bergsma JE. Surgery in and around the Orbit. CrossRoads. 2023.
Billing AB, Dengler J, Hardisty M, Chew HF, Kiss A, Fialkov J.A. Are We Overoperating on Isolated Orbital Floor Fractures? Plast Reconstr Surg. 2023 Sep 1;152(3):629-637.
Ozturker C, Sari Y, Ozbilen KT, Ceylan NA, Tuncer S. Surgical Repair of Orbital Blow- Out Fractures: Outcomes and Complications. Beyoglu Eye J. 2022; 7(3): 199-206.
Hsu CR, Lee LC, Chen YH, Chien KH. Early Intervention in Orbital Floor Fractures: Postoperative Ocular Motility and Diplopia Outcomes. J Pers Med. 2022;12:671.
Omura K, Nomura K, Okushi T, Tanaka Y, Otori N. Endoscopic Endonasal Orbital Floor Fracture Repair With Mucosal Preservation to Reinforce the Fractured Bone. J Craniofac Surg. 2021;32: 541–545.
Kuhnel T, Jagle H, Hosemann W, Webber R, The Vielsmeier V. Orbital floor fracture repair: the endonasal approach. Rhinology. 2017;55: 348-354.
Arosio AD, Valentini M, Canevari FR, Volpi L, Karligkiotis A, Terzakis D, et al. Endoscopic Endonasal Prelacrimal Approach: Radiological Considerations, Morbidity, and Outcomes. The Laryngoscope. 2021;131:1715-1721.
Kerdoud O, Aloua R, Kaouani A, Ousmane B, Slimani F. Repair of the orbital floor fractures: The endoscopic trans maxillary approach US minimally invasive approach: A case-report. Int J of Surg Case Rep. 2021;85:106279.
Vasile VA, Istrate S, Iancu RC, Pitiescu RM, Cursaru LM, Schmetterer L, et al. Biocompatible materials for orbital wall reconstruction ‑ an overview. Materials. 2022; 15:2183.
Shivam A, Enninghorst N. The Dilemma of Reconstructive Material Choice for Orbital Floor Fracture: A Narrative Review. Medicines. 2022; 9:6.
The Neto Silva J, box Saints MVT, with Carvalho PTB Noguiera, Filho LSL, Costa PJC. Treatment of blowout fracture with video-assisted surgery. Rev Bras Ophthalmol. 2019; 78(3): 188-91.
Saha M, The Curse A, Gadicherla S, Aramanadka C, Singh A, Varshney S. Combined Open Reduction and Transantral Endoscopic Approach for Internal Fixation of Orbital Floor Fractures: A Tertiary Care Center Experience with Decision‑Making Algorithm. J Maxillofac Oral Surg. 2024. https://doi.org/10.1007/s12663-024-02386-z
Lee YJ. Orbital floor fracture repair with implants: a retrospective study. Arch Craniofac Surg. 2021;22(4): 177-182.
Comments