SEPTORYNOPLASTY
I Made Nudi Arthana
Septorhinoplasty remains one of the most challenging operations in plastic and facial reconstructive surgery , a field that is gradually being developed by contemporary otorhinolaryngologists . Septorhinoplasty is a complex operation that requires precise preoperative diagnosis to select the appropriate surgical technique, partly because of its dual role and its primary importance for nasal function and facial shape.
LITERATURE REVIEW
Definition
Rhinoplasty is a reconstructive surgical procedure performed to change the internal and external structure of the nose with the aim of improving its appearance (aesthetics) or restoring the nose's ability to breathe (functional rhinoplasty). Meanwhile, septoplasty is a surgical procedure that only involves the nasal septum. Septorhinoplasty is a term used when rhinoplasty and septoplasty procedures are performed simultaneously. This procedure involves surgery of the bones and cartilage in the nose to improve the shape and structure of the nose (rhinoplasty) and straighten the septum (septoplasty). 5
Anatomy Nose And Proportion Face
The nose consists of skin, subcutaneous tissue, nasal skeleton and lining mucosa. cavity rice as well as septum rice Which limit cavity nose right And left. The nasal skeleton consists of a bone and cartilage framework. The bone framework consists of the nasal bone, frontal process, maxillary bone, nasal process, frontal bone and the bones that form the septum, namely the vomer bone and ethmoid bone. The cartilage framework consists of the upper lateral cartilage, lower lateral cartilage and septal cartilage. 6
The septum is the main basic structure of the external nose that supports the dorsum, columella, and tip of the nose. The septum also separates the nasal cavity, creating two distinct channels that allow air to move in a laminar manner, warm as well as moisturize air Which inhaled. Septum own three components main that is membranous, cartilage, And bone. Septum membranous consist of network fibrous And located on part most front from septum, between caudal tip cartilage quadrangular And crura medial cartilage lateral part lower. As the name suggests, the quadrangular cartilage is rectangular in shape and is located posterior to the membranous septum. The quadrangular cartilage attaches to the inferior maxillary crest, cartilage lateral on part superior, And septum bone part posterior; There is usually a thin caudal cartilage 1 to 2 cm long that rests on one side of the bony septum. The bony septum consists of the vomer, which is located inferiorly-posteriorly on the cartilage, and the perpendicular plate of the ethmoid (PPE), which is located superiorly and posteriorly. The ethmoid bone is adjacent to the skull base and the sphenoid bone and contains the medial and superior turbinates. The nasal bones are located on the dorsal aspect medial nose part on, superior to PPE And join with superior aspect of the upper lateral cartilage. 6
Another important anatomical concept is the internal nasal valve which is the narrowest part of the nasal passage - a triangular area just below the middle of the nasal dome. The boundaries of the nasal valve are the dorsal septum, the caudal border of the nasal cartilages. lateral on, And head turbinate inferior. Corner valve nose Which classically described as approximately 15 degrees, but often approaching 30 degrees; in about 50% of individuals there is also a submucosal collection of glandular and vascular tissue known as the septal swell body or septal turbinate , which appears to be a broader portion of the dorsal septum at the level of the internal nasal valve. 6
Two important points of septal articulation in surgical procedures are the junction of the anterior maxillary nasal spine and the " keystone area ". The keystone area is located on meeting between bone nose, cartilage quadrangular , cartilage upper lateral, And PPE; This is area important For stability And structure Which must handled with care during septorhinoplasty so as not to disrupt the supporting system of the nasal dorsum. This keystone area is located right at the cephalometric point called the rhinion. If disturbed, in a way technical will difficult For repair area keystone , and can result in nasal deformities such as saddle nose. 6,7
The cartilaginous and bony components of the septum are covered with mucoperichondrium and mucoperiosteum, respectively, which provide innervation and blood supply. This network of blood vessels allows humidification and warming of the air in the nasal cavity. The surface mucosa of the nasal cavity consists of from epithelium breathing pseudostratification. Epithelium olfactory accompanied by cell basal, And cell olfactory located more superior in near area gap olfactory on nasal cavity .
Picture 1. Anatomy framework nose from part front 8

n- Nasal bone
s- Upper edge of the nasal septum d- Triangular cartilage
f- Alar cartilage
a- Aperture piriformis
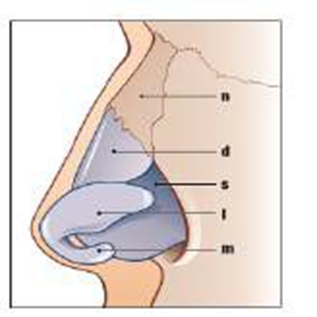
Picture 2 . Anatomy framework nose from view lower

d- Dome of the alar cartilage
l- Lateral crus of the alar cartilage
m- Medial crus of the alar cartilage s- Septum
Picture 3 . Anatomy framework nose 8
n- Nasal bone
d- Triangular cartilage s- Septum
l- Lateral crus of the alarm cartilage
m- Media crus of the alarm cartilage

Picture 4. Organ Odor, bone And cartilage septum nose; Viewed from Right side 6
The proportions of the face are determined primarily by the nasofacial, nasofrontal, nasolabial angles, and the length of the nose. Facial dimension analysis is performed based on topographic markers, such as the tip defining point (ape of the nose), glabella (metopion), and point Which define lips And chin (Picture 5). Findings This including in the pre-operative assessment by the surgeon and in determining the goals of surgery.

Gambar 5. Sepertiga wajah bagian atas, tengah dan bawah

Gambar 6. Perubahan proporsi wajah seiring bertambahnya usia yang mengarah ke bagian atas dengan menyusutnya garis rambut, bertambahnya panjang hidung, dan selanjutnya hilangnya gigi dan atrofi tulang rahang
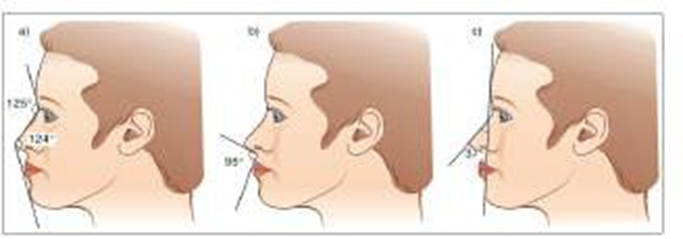
Gambar 7. Sudut penting untuk proporsionalitas wajah dengan nilai normal: sudut naso-frontal dan naso-mental (a), sudut naso-labial (b), sudut naso-fasial (c)
Indication And Contraindications
Indication
A number of indication septorhinoplasty that is as following 6 :
There is anatomical displacement of the nasal bones, septum, or other structural abnormalities that cause mechanical obstruction of the nasal airway.
The existence of deviation, obstruction, or deformity septum And pyramid nose Which severe or unresponsive to conservative medical management for at least 3 months, including intranasal corticosteroids and immunotherapy
Reconstruction deformity nose post trauma And reconstruction septal perforation
Disturbance aesthetics including reconstruction abnormality nose congenital complex ones such as cleft lip nose .
Augmentation/reduction back rice on 2/3 nose
Tip projection, twisted nose
Structural grafting And revision rhinoplasty
There is condition other like epistaxis repetitive, obstructive sleep apnea, sinusitis, and painful face and/or Sick head consequence septal spurs Which touch with turbinates (Sluder's syndrome).
2.3.2 Contraindications
There are several contraindications for septorinolasti including disease accompanying on patient like rhinosinusitis or vasculitis, or there is conditions where adequate medical therapy has not been applied. Adequate therapy such as the use of nasal sprays to reduce chronic inflammation can relieve symptoms of nasal obstruction so that surgical intervention is not needed. 6
Active use of illicit drugs during the perioperative period, especially intranasal cocaine, is strongly discouraged. The vasoconstrictive and damaging effects mucosa from cocaine can trigger complications like perforation septum and delayed healing, which may ultimately lead to dorsal nasal collapse. so that result in abnormality form nose saddle nose . Patient ensure that you have not used any illegal drugs for at least 6 to 12 months before surgery, and a toxicology test may be required to ensure compliance . patient. 9 Similar precautions Also should be done on patients who show signs of rhinitis medicamentosa. Nasal decongestant sprays that cause vasoconstriction should also be avoided for a period of time before surgery, although these drugs may help limit intra- and postoperative bleeding. 6,9
Patients with unrealistic expectations regarding the aesthetic or functional results of septorhinoplasty should not be offered surgery. without counseling extensive pre-operative. Surgeons and Patients need to share achievable expectations, as this will increase satisfaction. patient And expert surgery post operation. Thus also, they Which experiencing deviation and deformity of the nasal septum and pyramid, but limited functional symptoms, may only feel a little benefit from surgery. 6
Patient comorbidities, functional status (ASA grade), and age all need to be considered to determine whether general anesthesia is safe and whether the patient can tolerate the postoperative recovery process. 6
Inspection Pre- Operative
Anamesis
A complete history regarding the nature of the nose and nasal-related symptoms should be obtained. Symptoms of sinonasal pathology or other systemic symptoms, including allergies, should be evaluated. Scoring systems such as the Nasal Obstruction Symptom scale Evaluation (NOSE) can used For evaluate degrees obstruction nose. Patients with low NOSE scores are not recommended to undergo surgical procedures. 10
A thorough history is also important to determine whether concomitant factors may contribute to or cause the obstruction, such as trauma, rhinosinusitis, allergies, vasculitis, illicit drug use, chronic decongestant use, autoimmune disease, or malignancy. In these cases, adequate medical therapy (eg, intranasal corticosteroids for chronic allergic rhinitis) should be offered before considering surgery. 6 If the patient is a smoker, smoking cessation should be considered, although smoking has not been shown to worsen surgical outcomes. History operation nose or sine previously, problem with anesthesia previously, or condition bleeding Also must dug up For prevent the occurrence complications when the surgical procedure is performed. 6,10
Inspection Physique And Support
Inspection comprehensive including inspection complete head And neck should be done, followed with rhinoscopy front with speculum nose. Nasoendoscopy A flexible rhinoscopy may be performed to look for signs of sinonasal disease or a posterior nasal mass, especially when anterior rhinoscopy is inconsistent with the patient's history (eg, symptoms of severe nasal obstruction with normal-appearing turbinates and a centrally located anterior septum). When evaluating the nasal septum, the examiner should look at the quality of the mucosa (assessing for signs of inflammation) and size as well as characteristic turbinates, specifically turbinate inferior. If access bad Due to excessively large turbinates, turbinoplasty may also be indicated. 10
The septum should be palpated to evaluate the size, location, and nature of the deviation, noting specifically whether cartilage or bone is visible and whether there is any perforation, dislocation, or bony spurs . If patient own history previous septoplasty, it is important to palpate the septum using a cerumen curette or cotton-tipped applicator to evaluate the amount of remaining cartilage. in in septum. Inspection external must done And take note presence of additional deformity, dynamic collapse of the alae on inspiration, and degree of nasal tip support. Cottle maneuver should be performed to assess for internal valve stenosis. A thorough examination will help determine the indication for surgery, level the difficulty, as well as approach And technique What Which most suitable for patient. Photography nose with picture static And dynamic from side frontal, three-quarter, lateral, base ( worm's eyes ), And dorsal ( bird's eyes ) must documented during physical examination, before surgery and after the patient undergoes a surgical procedure. 11 Inspection support like Photo plain OS nasal And water view can also help in establishing the diagnosis. 10
Material Graft
Grafts can be broadly categorized into autogenous, homologous, and alloplastic types. Injectable agents such as hyaluronic acid are sometimes used for enhancement. 2,3
Graft Autogenous
grafts are taken from the patient and include cartilage, bone, and various soft tissues, such as the perichondrium and temporalis fascia. Autogenous cartilage is material graft structural choice Because convenience the engraving and reliable long-term results, with low rates of infection, resorption, and extrusion. Autogenous grafts also avoid the potential risk of immune response or contamination virus. Graft cartilage useful For give construction structural and create contour. Representative septal, auricular, and costochondral grafts are shown in Figure 8. When destroyed, cartilage can still survive and support the growth of surrounding cartilage. 2
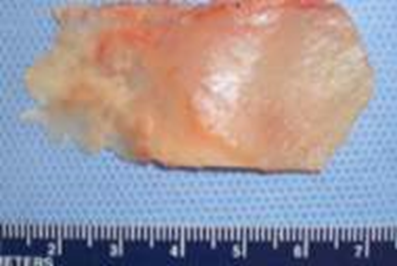
Figure 8 Septal Cartilage
Septal cartilage is the most common graft material used in surgery. nose primary, Because the taking Which easy And lack of morbidity in location donor in a way functional or cosmetics. Besides That, cartilage septum very versatile in graft function and has reliable long-term results. It is useful for spreader grafts , columellar supports, alar rims, augmentation dorsal, And graft edge alarm. Cartilage septum Also can destroyed to add volume or smooth the contour transition. When harvesting septal cartilage, it is important to maintain 1.0 to 1.5 cm of L-shaped caudal and dorsal support. Septal cartilage is often limited in the setting of revision rhinoplasty. For major revisions, an open rhinoplasty approach may be used in which bilateral submucoperiosteal and submucoperiosteal flap elevation is combined with distribution cartilage lateral superior. With approach This, septum And The nasal dorsum is in the “ ouvert au ciel ” (open to the sky) position, resulting in exposure Which wide For diagnosis, collection material remainder structure, and treatment of structural abnormalities. Auricular cartilage is commonly harvested for use in revision rhinoplasty when the septal cartilage is inadequate. Auricular cartilage is softer than septal cartilage and has a curved shape. This curvature and flexibility make auricular cartilage a less desirable graft material for certain purposes, such as when a spreader graft is needed to support a thin columella. 2,3

Picture 9. Cartilage Konka.2

Picture 10. costochondral Costae. 2
grafts provide sufficient graft material for rhinoplasty surgeons. For nose Which lack structure. Cartilage costa possibility large is required after a traumatic injury that is damaging or after excessive resection during a previous reductive rhinoplasty. The quality and quantity of costal cartilage that is very Good make it place donor choice when cartilage septum And auricular is insufficient. The main disadvantages of costal cartilage are its tendency to buckle, scarring at the donor site and postoperative pain, potential stiffness and calcification of the cartilage in adult patients, and additional operative time. 2,3
grafts for rhinoplasty are most useful for grafting the upper third of the nose and are obtained from the calvarium, costal bone, or, more commonly, seldom, Christ iliac. Bone calvarial, Which is bone membranous, resistant to resorption And maintain contour more effective compared to bone iliac, which is endochondral in origin. Calvarial bone is also associated with less donor site morbidity, although complications of cerebrospinal fluid leak, sagittal sinus laceration, intracranial injury, and subdural hematoma have been described. Calvarial bone is harvested as a split calvarial bone graft through a hemicoronal incision over the parietal skull. Costal cartilage is preferred over costal bone grafts . Although autogenous bone is well known in the rhinoplasty literature, the disadvantages of this donor site are its susceptibility to fracture, greater difficulty in carving and securing the graft , and a tendency for the graft tip to loosen. 2,3
A variety of other autogenous materials are also useful for soft tissue augmentation in rhinoplasty, especially as adjuncts to structural grafts . Examples include costal perichondrium (collected at the time of costochondral graft harvest ), temporal fascia, and fibroadipose tissue from the post-auricular area. can flattened become sheet thin with tool fascia otological. Each of these tissues can be harvested with little or no additional morbidity at the donor site. These grafts can provide significant aesthetic benefits by softening framework interface network soft. Most general, network This used to disguise cartilage grafts or to correct minor contour irregularities. In operation nose revision, network soft can used For to coat thin and atrophic skin due to scarring and contracture. This soft tissue reduce risk dextrusion graft , prevent formation boss , protect the soft tissue of the skin sheath above it, and improves the quality of the skin sheath. overall. 2.3
Graft Homolog
The most commonly used homografts are irradiated costal bone for structural grafts and acellularized dermal matrix for soft tissue augmentation. In general historical, graft This, Which originate from corpse man, proven not enough predictable compared to network autogenous in his ability oppose resorption and bending; however, the experience is mixed. The potential risk of human pathogen transmission is also a concern for patients. Nevertheless, this graft material is useful in selected patients who are poor candidates for autogenous tissue harvesting or who do not wish to have an additional donor site. Situation This seldom happen. Homograft cartilage costa taken from corpse that have been screened and irradiated to at least 30,000 Gy to reduce antigenicity. These grafts are associated with low rates of infection and destructuring, although soaking them in antibiotic solution prior to use is still recommended. Acellularized dermal matrices have been shown to have significant resorption within the first year, although this resorption tendency may stabilize thereafter. Because of these limitations, acellularized dermal matrices are more appropriate for graft camouflage and contour smoothing under thin skin than for volume enhancement. 2,3
Alloplasty
In recent years, alloplasts have become more popular due to their relative ease of use, unlimited supply, pre-designed or easily adaptable shapes, and lack of donor site morbidity. Most alloplast is polymer, Which is chain long subunit More commonly used implants include expanded porous polytetrafluoroethylene (e-PTFE; Gore-Tex), porous high-density polyethylene (PHDPE; Medpor), polyester fiber mesh (Mersilene), and silicone, which is primarily used in Asian patients. Which own skin thick. Response biological Which caused by host after The use of allografts is influenced by the chemical composition and physical characteristics of the graft . Implantation all alloplast cause response inflammation. On phase I, neutrophil and macrophages recruited, And material protein to coat implant. Fibroblasts keep collagen, and phagocytosis occurs in implant particles smaller than 60 micrometers; particles larger than 20 micrometers cause macrophage death and secondary release of local inflammatory mediators. 2,3
Size pores influence trend growth fibrovascular into and risk of infection. Alloplasts with pores larger than about 50 micrometers will show growth network to in, with pores larger ones support larger inward growth. PHDPE has pores big Which allow network soft And growth bone to in limited. This PHDPE graft is difficult to remove, but is also more resistant to infection. On the other hand, e-PTFE own pores Which more small so that more easy removed after implantation. Silicone forms a fibrous capsule without ingrowth and carries a persistent risk of dehiscence throughout the patient's lifetime. Not all agent synthetic capable endure. Net polyamide (Supramid), Which demonstrated excessive degradation and resorption in animal models, is now of historical concern. Polytetrafluoroethylene (Proplast) demonstrated fragmentation under mechanical stress in temporomandibular joint surgery, leading to its removal from the United States market. 2,3
Technique installation graft
Some special graft techniques in septorhinoplasty are used to repair structure nose And fulfil need individual patient. Following is a brief explanation of these special techniques 2,3 :
Septal Extension Graft :
Technique This involving use graft (usually from cartilage septum) to extend or repair part tip nose. Graft This placed in septum tip For give buffer addition And help repair nasal proportions. Septal extension graft is useful for treating short noses or those with structural deficiencies at the tip.
Spreader Graft :
A spreader graft is a graft that is placed between the lateral cartilages of the nose. (cartilage lateral) And septum. Purpose is For repair septal deviation And open or to widen channel breath nose. Spreader graft often used to correct a narrow nose or a nose that has collapsed on the lateral side.
Alarm Rim Graft :
graft is placed on the alar margin (outer part) to repair or augment the alar structure edge nose. Used For increase deficit edge nose or repair structural weaknesses in the nasal alar.
Columellar Strut Graft :
graft is placed under the columella (the part that connects the nose and lower lip) to provide additional support, useful for repairing a weakened nose or preventing deformation of the columella after rhinoplasty.
Tip Graft (L-tip, Shield Graft )
A graft placed at the tip of the nose (tip) to improve the shape, projection, or symmetry of the nose. Different types of tip grafts include L-tip graft (to correct a crooked nose), shield graft (to improve nasal contour deficits).
Stages Septorhinoplasty
Preparation Patient
Equally important are the techniques, maneuvers, and procedures you will use. in surgery is preparation patient For surgery. Important for surgeons to get a comfortable operating process, and for patients to feel comfortable after operation. After enter to House Sick, patient brought to room operations and return to House 6-8 O'clock after operation. Xylometazoline spray nose used for vasoconstriction of the septal mucosa. The spray is administered to the patient who is asked to take a deep breath while pressing the pump into each nostril and to clear the nose afterwards. In this way the spray acts homogeneously on the mucosa. Using the spray 30 minutes before surgery ensures a bloodless septoplasty and reduces systemic absorption of the septal injection. It also eliminates the need for the use of adrenaline-containing nasal packing during surgery.

Picture 11. Use Xylometazoline (A), appearance mucosa The septum shows decreased vascularization of the septal mucosa (B). 19
Position patient, operator And intubation tracheal
Before any surgical procedure, medical clearance should be obtained, including preoperative risk stratification and medical optimization. Preoperative photographs with static and dynamic images from the frontal, three-quarter, lateral, base ( worm's eye ), and dorsal ( bird's eye ) sides as well as nasal shape, facial asymmetry, and the effect of a smile on the nose should be adequately documented . 11
The patient is positioned supine with the shoulder roll position (sniffing position) . The chin patient must seen And tracheal tube positioned stay away expert surgery with angle 45°. Make sure tube intubation No interesting lips. If hose positioned in midline as a reference point. The chin remaining in the visual field will provide greater control. The intubation tube pressure is measured during surgery. This reduces throat pain after surgery. The patient is positioned in position Trendelenburg backwards, with head extended 20–30° so that parallel with floor. Position This allow hips is at on position lowest. Be sure to have a hydraulic bench that can be controlled by foot. The operator should evaluate the nose from various angles by adjusting the height as needed during the operation. In addition, the cartilage can be sutured more precisely while sitting. Adrenaline solution injected into the nose provides vasoconstriction And surgery can done with see the details. However, the increase pressure blood And pulse pulse consequence effect systemic adrenalin against vasoconstriction local. By Because That, need done control pulse pulse and blood pressure. A single dose of intravenous antibiotics can be administered before the patient undergoes surgery. A single dose of intravenous steroid injection (eg, dexamethasone 8 mg) can help reduce swelling. A single dose of intravenous tranexamic acid (10 mg/kg) can help reduce intraoperative bleeding. The best parameter that reflects pulse rate and blood pressure instantly is the end-tidal CO2 pressure (EtCO2). When injecting local solutions, ensure that EtCO2 remains between 30 and 34 mmHg. If EtCO2 increases, take a break from the injection until the pressure has decreased. 19

Picture 12. Patient positioned in position Trendelenburg backwards, with the head extended 20–30° (A) and the operator on the upper side of the patient (B). 19

Picture 13. Applying povidone iodine (A), cut hair nose
with knife surgery (B).
Remove hair nose with knife. Giving povidone iodine will make it easier for the knife to move on the mucosa.
Anesthesia
Local anesthesia is infiltrated bilaterally in the sub-mucoperichondrial plane, using 1% lidocaine with epinephrine (1:100,000) until the mucosa becomes completely pale. This can help in the hydro-dissection process in addition to providing analgesia and hemostasis. 6 General anesthesia or intravenous techniques (e.g. Propofol) are recommended for surgery. open septorhinoplasty. If general anesthesia is used, muscle relaxants may be an option. 6,11
Figure 14. Stages of local anesthetic injection (A) Both sides of the caudal septum (B) location incision Which planned For tip nose And in above the lateral crura (C) Deep valve (D) Injecting under the perichondrium starting from the angle of the septum facilitates subperichondrial dissection (E), Top of the radix mucosa (F), Above and below the piriform aperture (G), Perpendicular mucosa of the ethmoid bone (H). 19
Draw pattern
A photo of the nose can provide further information. Below you can see drawing created on an electronic drawing tablet within 5 minutes minute, see edge cartilage And picture line mainly. Use line thin for concave and convex shapes. In this way, the cartilage anatomy is visible without lifting the skin. 19

Picture 15. Photo patient pre-operation on Which analyzed in a laptop.19

Picture 16. Design nose with Photo details patient on side front (A), upper side (B), lateral side (C) of patient undergoing surgery. 19
Marking
Marking the planned tip on the nose, draw two to three darts on the cheeks pointing to this point. These lines guide the adjustment of the tip position. Determine the lateral crus steal according to the lines . This, decide position dome Which Correct with do lateral crural steal until the tip rotates to the previously marked point. In the shaded photo, the tip of the nose is then found. Mark the tip to be planned on nose patient. Draw a picture three line Which show point This. Do This before start operation, Because form nose will changes with dissection and resection. If you have a tip reference, you can decide more easily in surgery. 19

A standard set of septorhinoplasty tools usually includes the following. Please note: that doctor surgery only can use part small of this instrument during surgery, depending on the technique performed 6 :
Light head
Speculum nasal hartmann / vienna
Speculum nasal cottle
Speculum nasal Killian (3 size)
Retractor Killian
Hills elevator
Knife #15 on scalpel handle bard parker #7
Scissors bent cottle
Scissors nasal gorney
Forceps jansen- middleton
Forceps nasal blakesley
Forceps nasal Takahashi
Forceps nasal blakesley- wilde
Forceps nasal dressing lubet- barbon
Tip suction ferguson or Frazier
Forceps bipolar diathermy
Forceps adson- brown
Forceps bayonet cushing- brown
Forceps nasal dressing Jansen
Forceps lateral lower cottle
Applicator cotton
McKenty raspatory
Freer chisel
Elevator free
Knife septum free
Elevator Pierce
Elevator cottle
Elevator Woodson
Cottle chisel
Cottle metal mallet
Forceps backhouse towel
Needle holder
Medicine cup
Hopkins rod, light source, And stack (If using an endoscope)
Silastic Splints
Thread gut chromic 5-0 and 4- 0
Mupirocin ointment
Technique Surgery Septorhinoplasty
The technical modifications required for septorhinoplasty can be performed endonasally (without external incisions), and openly (with a small incision across the columella). 12
Endonasal Septorhinoplasty
Elevation mucoperichondrium flap
A nasal speculum is used to expose the caudal edge of the cartilaginous septum. An incision is made using a #15 blade along the caudal edge to expose the cartilage. Commonly, the incision used is a hemitransfixation incision (vertical incision through one side of the membranous septum) or a Killian incision. (incision vertical Which located more posterior, in on cartilage quadrangular ) (Image 18). If septoplasty done simultaneously with open rhinoplasty, The septum can be seen from above after the upper lateral cartilages are detached from the dorsal quadrangular cartilage. 6
Surgical scissors and a Freer or Cottle elevator are then used to widen the sub-mucoperichondrial plane and cut posteriorly to expose the cartilage quadrangular , PPE, And vomer. Inspection cartilage It is very important to ensure that the mucoperichondria flap elevation is well vascularized and strong; the quadrangular cartilage usually appears pearly white/blue. At this stage, care must be taken not to happen perforation on mucosa, especially If required surgery on bone spur or deviation. 10 Bilateral and opposing perforations can lead to postoperative septal perforation. The second flap on the contralateral side can then be raised. through incision Which The same. When will reach side Which more Far posteriorly , a longer nasal speculum is required to obtain good visualization.6

Figure 18. Incisions in septoplasty. (A) Kilian incision and hemitransfixation incision for mucochondrial flap. (B) Septotomy with L-strut preservation. Which adequate. (C) Septotomy done on intersection bone vulnerable 12
Correct septal deviation
Evaluation is done on the location, direction, and nature (cartilage/bone) that is deformed. Various instruments can be used to incise the septum, and are sometimes used in combination. Knife, Freer elevator, Jansen-Middleton forceps, or forceps Takahashi used For lift bone deviated cartilage. To maintain stability of the dorsum and tip of the nose, the quadrangular cartilage (L-shaped strut) is preserved (dorsal and caudal edges). Therefore, the posterior aspect of the cartilage is often the area of removal. If the deviation involves the L-strut, extracorporeal septorhinoplasty or approach open with graft Possible required. The dorsal and caudal parts of the L supports, as well as their attachments to the bones, must remain intact. wide 10 until 15 mm For ensure strut nose part outside adequate. Twisting movements are often performed to remove cartilage or bone; avoid excessive twisting outside the anterior-posterior axis as this can cause cribriform plate fractures and potential cerebrospinal fluid leaks. 6,13
Cartilage Which has lifted must saved in solution normal saline or cloth gauze surgery Which wetted with solution normal saline. Piece cartilage The original can be reshaped and used to reinforce the L-support if necessary or used as a graft in rhinoplasty. 6
Closing
The mucoperichondriacal flap is repositioned against the septum. Interrupted sutures using absorbable sutures (such as chromic gut ) are used to close the incision. Hecting mattresses , or quilting sutures , are often made through the septum to close the dead space and adjust the size of the flap to avoid postoperative hematoma accumulation. If the mucoperichondriacal flap still intact on end operation, a number of expert surgery will making a small incision inferior to one flap to facilitate drainage of any fluid that may have accumulated in the septum. Some surgeons prefer to use a septal stapler rather than hand- applying quilting sutures. At this stage, a silastic splint is sometimes required. The flap is cut to size, placed adjacent to the septum, and sutured transseptally so that easy issued in clinic take care road. Splint This aiming to prevent adhesions to the conchae if the conchae are hypertrophied or if turbinoplasty has also been performed. Antibiotic ointments can be applied intranasally. 6
Incision And dissection on rhinoplasty
Subperichondrial and subperiosteal dissections are key elements in proper healing after rhinoplasty. Less fibrosis is observed in these areas of dissection. The perichondrium or periosteum left on the skin side of the dissection serves as a strong cover against changes occurring in the osseocartilaginous framework . Placement of the incision and technique of dissection are important for ease of dissection on field This. Discussion This focus on tip And tricks about incision and dissection. 19-20
Hemitransfixation and Transfixation
Using a transfixation incision on the long nose and a hemitransfixation incision on the remainder. The incision made from the membranous septum enters ligament line middle “Pitanguy” until pass integrity ligaments.
Study previously make incision appropriate in on caudal septum And leaving a 0.5 mm wide portion of the caudal septum attached to the Pitanguy ligament . Leaving the caudal portion of the septum wider makes it more difficult to suture it. return in end operation. Whereas For incision transfixation to internal valve area, made with a 3-4 mm posterior incision along the upper lateral cartilage edge. Intercartilage incision is not made, thus improving mucosal healing. 20

Picture. 19 A)Incision on caudal septum 0.5 cm with knife surgery #15 B) so that it adheres to the perichondrium on the opposite side. C) The cartilage left attached to the Pitanguy ligament through the membranous septum can be called a “posterior buttress”. D) At this stage, the septum is dissected on both sides in the subperichondrial plane. E) Suturing the mucosa to the septum. 20
Entering Nasal Back from Corner Septal
Using sharp scissors , separate the posterior struts completely. from corner septum. After cartilage separated 3-4 mm, move going to nasal dorsum from the angle of the septum, then down to the upper lateral cartilage. At this point the caudal edge of the nasal dorsum perichondrium will be visible. This is the most appropriate For is at in lower perichondrium. If the scissors not enough sharp, will have difficulty getting under the perichondrium. 20

Picture 20. Incision on caudal septum. 19
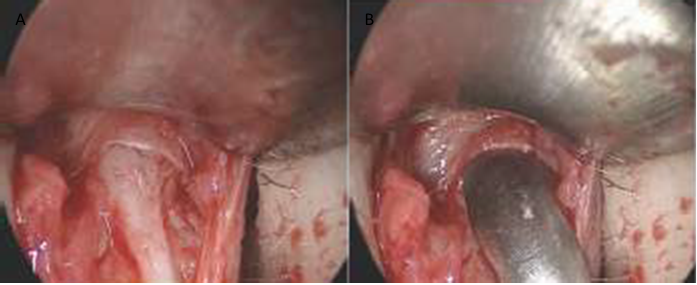
Figure 21. Endoscopic photograph showing the entry of the subperichondrial plane from the anterior septal angle. Using sharp-tipped scissors the posterior strut is completely separated from the septal angle (A). After the cartilages are separated by 3-4 mm, the going to back nose from corner septum done until cartilage upper lateral (B). 19

Picture 22. A) Moving elevator to side, dissection perichondrium upper lateral cartilage and stops at the ligament. B) continue with dissection of the nasal tip cartilage. 20
Incision Infracartilaginous And Autorim Flap
The incision is made from cartilage tip (infracartilaginous incision). If there is excess in part caudal, so will done auto rim flap . Install double hook and turn it over end hole nose with finger middle. Edge crural lateral can seen at the incision site 6-7 mm long and 1 mm deep will be made. When approaching dome, will difficult For visualize edge cartilage. Keep it up direction of the first incision and continue to the caudal part of the dome, ending 3–4 mm before the dome. After the lateral crural steal , continue the incision along the caudal edge of the medial crus. The incision is completed 3–4 mm before the foot plates . Another option is to make a medial and lateral crural incision and connect them. Make an intracartilage incision on the lateral crus. Turn the columella upside down with your fingers and cut the mucosa along the medial edge of the crus. Place a double hook at the apex of the nostril and turn it upside down. Then join the two incisions. 19
Dissection Subperichondrial Lateral crural
Subperichondrial dissection may facilitate the use of the spreader g raft flap technique on the dorsum; however, all surgeons reported that their dissection was performed in the subperichondrial plane on the lateral crus . If making dissection subperichondrial Which Actually can with clear write in bonevulnerable with pen surgery, like write in on paper with pen. Moment dissecting subperichondrially on the lateral crus, as in subperichondrial dissection of the septum, one can clearly see the perichondrium on the covering. Because the muscle and perichondrium remain on the cartilage when subperichondrial dissection is not used, the marking pen ink will spread. Subperichondrial dissection is very easy to perform with tool surgery Which Correct And technique Which in accordance. Required time 10– 15 seconds to get into the correct field and surgery is much faster. Key point For dissection crural lateral is point come back crural lateral. Nurse must pull the hook to lower with gentle. Pull return skin For see edge bone vulnerable to use tool with end sharp. Cut with knife until reach the cartilage. When reaching the cartilage, hold the knife upside down and make an incision in the perichondrium. 19-20


Figure 23. Making the auto-rim flap, making the marker (A), The auto-rim flap incision should be made at a distance of 2–3 mm from the dome (B), Place the double hook at the top of the nostril and invert then join the two incisions (C), enter the subperichondrial plane with sharp-tipped scissors through the long axis of the cartilage for 2–3 mm (D), After passing through the dome , subperichondrial dissection crural medial become more easy. Split area This with Daniel's elevator and stretch the ala with the retractor (E). 20
Merge Dissection Tip and Dorsum
The dissection of the dorsal cartilage is complete. The tip surgery is also complete. Now second field surgery This will united on region scroll. 19

Picture 24 . Dissection tip And dorsum. 19
Dissection periosteal
The periosteum is cut with an elevator and a subperiosteal plane is inserted. Insert a small retractor under the periosteum, press the skin flap with the underlying periosteum with your fingers, and stretch downward. 19-20
Figure 25. Stages of periosteal dissection, Insert a small retractor under the periosteum, grasp the skin flap with the underlying periosteum with a finger, and stretch it downwards (A), With a periosteal elevator, scrape the perichondrium and periosteum in edge inferior bone (B), With formation tunnel, direct vision surgery can be performed up to the radix. Perform deeper surgery with the Aufricht retractor (C), In this endoscopic view, an incision in the periosteum of the left maxilla can be seen (D), Dissection of the right nasal bone.
Periosteum cut with elevator (E), Transition between perichondrium and the periosteum can be seen (F). 19
Turbinectomy
Turbinectomy surgery may be necessary in patients with respiratory problems. Preoperative endoscopic examination will reveal the need for intervention. turbinates. On study previously with apply resection submucosa turbinates at 2 0%. After infiltrating the turbinates, a small incision is made and the submucosal cavernous tissue is removed. Bone interventions include lateralization of the turbinates and partial bone excision, which can be performed by removing small pieces of bone. Techniques This Also can done with use with radiofrequency monopolar or electrocautery. Splint nose silicone internal installed after intervention And removed on the fourth day after surgery.

Fig. 25 Steps of turbenectomy with submucosal resection, a small amount of local anesthetic solution with epinephrine on the enlarged concha and wait a few minute (A),. use knife surgery, for incision shaped C measuring 4 mm on the anterior turbinate (B), Cut the cavernous tissue between the mucosa and bone (C). 20
Solution anesthesia local with epinephrine on concha Which hypertrophy And Wait a few minutes. Gently advance the conchae so as not to tear the mucosa. Using a scalpel, make a 4 mm C-shaped incision on the superior turbinate (the concavity of the C should face laterally). Perform an elliptical resection starting from the superior turbinate. Cut the cavernous tissue between the mucosa and the bone. Procedure This useful although applied on depth 3–4 cm just. With response 2 mm or elevator Cottle , cut second side bone. Spin respond 90°, move to over the bone and try to break the bone with a controlled back and forth motion. Rotate the respat 90°. Break off small pieces of bone by moving the respat over the bone. Aspirate the free portion and then remove the bone pieces. 19
Septoplasty
Septoplasty is part integral from operation nose. Septoplasty L Classically removes a large amount of cartilage, does not immediately correct the deviation, and makes revision rhinoplasty difficult if necessary. The portion of the septum that causes the deviation is usually the excess base portion. Removing this excess is often sufficient to correct the deviation. Split the mucosa only at the base, and remove the excess cartilage and the deviated maxillary spine portion. On the other hand, a low septal strip requires dissection of the entire septal mucosa and ethmoid. The deviated portion of the ethmoid that is in contact with the middle turbinate must be corrected. In addition, there is no need to correct a high septal deviation. Extracorporeal septoplasty should be performed in patients with severe septal cartilage abnormalities. 19-20

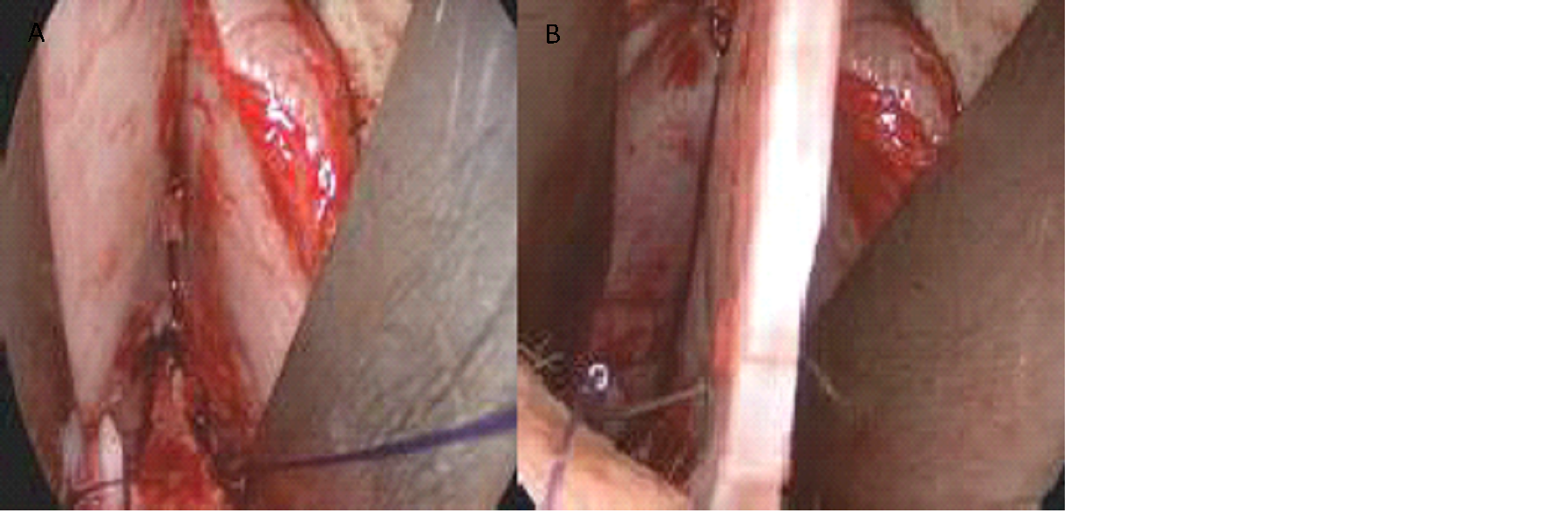
Picture. 27. Resection on septoplasty, septoplasty extracorporeal (A), illustration of septal resection (B)
On part dissection (Incision And Dissection on Rhinoplasty), discuss about the transfixation incision and posterior strut technique. This posterior strut will be left in place in columella And septum dissected. When buffer posterior made,
cephalic edge of the septum becomes thick which is an easy place to enter the subperichondrial plane. Perichondrium incision with the back of the knife. Perichondrium dissection with a thin Cottle or Daniel elevator. Without removing part excessive in base septum, No There is procedure (even septoplasty L) which can correct the axis deviation. The septum is dissected on both sides of the resection area. If it is necessary to print the cartilage, incise according to the excess part of the septum, cut it with a 3 mm lateral osteotome and remove the cartilage with a Cottle elevator or a Çakır perichondrium elevator , being careful not to damage it. After removing the curved or excess cartilage, dissection periosteum peak jaw on. Don't dissect all in all before resection because it can injure the mucosa. Soft tissue dissection with a Cottle elevator . The height of the foot plate decreases as the amount of dissection increases. excess on both sides using a 4 mm chisel or cut the bone with bone scissors. Leave a 2 mm gap between the base of the septum and the back of the jaw on anterior. Periosteum And network perichondria Which left behind on mucosa will fill the space. Correct the deviation of the ethmoid bone. At this stage stabilize the septum to the maxillary spine midline using 5/0 PDS. Since blunt dissectors are used when removing excess cartilage from base nose, network soft Which remaining on bone behind jaw on anterior is still sufficient for suturing and stabilization. If the septum is mobilized later during operation, installation to base will become more difficult. Incision transfixation is a good incision to attach the septum to the base. If the node remains in between septum And bone behind in distance 2 mm, so No will cause any suture reaction. If the gap is greater than 2 mm, this space can be filled tying more knots. The curved septum and vomer bone can be cut with forceps . Ayhan who is a tool designer at Medisoft perfected the power arm and the tip of the instrument to be used in confined spaces. When the septum surgery is complete, check the nasal passages for any obstruction. If there is no problem, insert a silicone splint. Sometimes the bone pieces or bone vulnerable can tear mucosa And caught channel nose. Network Which stand out This No will easy epithelialized And can cause bleeding, crusting, and odor in the nose because it can still be blocked. If there are no problems, insert a silicon splint. 19-20


Picture. 28. Stages septoplasty. Incision perichondrium with side behind the knife (A), dissect on both sides of the resection area (B), Open the excess septum, cut with a 3 mm lateral osteotome and remove the cartilage with
elevator Cottle (C), After remove bone vulnerable Which curved or excessive, dissection of the periosteum of the maxillary apex. Do not dissect completely before resection Because can to hurt mucosa (D), Incision periosteum anterior maxillary spine (E), Correction of ethmoid bone deviation (F). 19
Picture. 29. Sewing cartilage with mucosa, needle entered on side of the septum, until it penetrates the other side (B). 19
Open Septorhinoplasty
Approach modern For rhinoplasty open focus on change gradually on cartilage And framework bone. Following steps in open septorinoplasty: 11



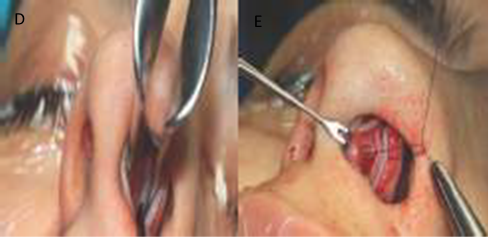
Figure 30 . Stages of open septorhinoplasty, incision in the columella (A), dissection in the subperichondrial (B), cut perichondrium bone vulnerable lateral on with performing a right and left swiping motion similar to the closed approach (C), place two marker sutures and cut between them to reach the septal angle.
Find out perichondrium as high as corner septum And enter in underneath using an elevator (D), when reaching the bone, cut the periosteum and perichondrium with a knife (E), Pitanguy's roll and ligament as seen in open approach subperichondrial dissection (F), Bone dissection begins laterally with a periosteal elevator (G). 19
The open septorhinoplasty approach involves making an inverted V-shaped mid-columellar incision , which is performed where the lower cartilage is closest to the skin to avoid postoperative scar visibility and contracture. With help hook skin And tool surgery sharp (for example scissors
converse ), the mid-columellar incision is transitioned into a marginal incision carefully to avoid injury to the medial and lateral crura. The soft tissue envelope is then reflected superiorly in the relatively avascular supraperichondrial plane to expose the upper lateral cartilage (ULC). At this point, the ULC dissection is transposed to the sub-perichondrial plane using sharp dissection. A periosteal elevator (eg, Joseph elevator) is then used to elevate the periosteum over the nasal bones to the nasofrontal angle. The lower lateral cartilages are then divided in the midline to expose the anterior septal angle (ASA) in preparation for septoplasty and/or septal cartilage harvest.
After the columella incision, continue between the medial crura without cutting the bone. vulnerable. Cut aponeurotic muscle superficial (SMA) in a way shallow. Open the perichondria window on the medial crus and begin scraping upwards.
Continue with subperichondrial dissection of the lateral crus . Can begin dissection from crus lateral And Then cut columella. A number of expert surgeons consider dissection from the lateral crus towards the dome to be more practical.
Make two marking stitches and cut between them until you reach corner septal. Find out perichondrium as high as corner septum And enter beneath it using a perichondrium elevator
The midline ligament of Pitanguy can be easily visualized midway when the end cartilage is dissected subperichondrially.
Dissect the perichondrium of the upper lateral cartilage by performing a right and left swiping motion similar to the closed approach.
The scroll and ligament of Pitanguy as seen in an open approach subperichondrial dissection.
When you reach the bone, cut the periosteum and perichondrium with a knife. There is a sharp bony angle lateral to the paramedian groove. Scrape that corner with a periosteum elevator and begin to elevate the periosteum with ease.
Septoplasty : Corner front septum Which seen, And pocket sub-mucoperichondrial which formed in part caudal nasal spine And in posterior on intersection bilateral septal cartilage. If the surgeon anticipates graft spread, the upper lateral cartilage should be removed from the dorsal septum to the nasal bone. At this point, the septal cartilage can be carefully removed to leave a 1.5 cm L-shaft to maintain adequate structural support. Bony deviations and/or bony spurs are removed using basic septoplasty principles. In addition, the “ swinging-door ” maneuver with excision cartilage septum inferior-caudal Which repetitive can done to correct caudal septal deviation. 14
Contour tip nose : Expert surgery rhinoplasty must understand various technique hecting in tip-plasty such as transdomal sutures, interdomal sutures, lateral crural mattress sutures, and columella-septal sutures. Each suture technique has its own variations and subtleties. In addition to suture-based techniques, softened cartilage grafts and/or cartilage perichondrium can be sutured to the dome to add projection or camouflage to the tip. Other techniques used to address tip/supra-tip features include cephalic trim , cephalic turnover flaps , and lateral crural strut grafts , which are useful in correcting lateral crural convexity or malposition. Cartilage cutting techniques (eg, vertical dome division, lateral crural overlay, and medial crural overlay) are also tools Which powerful For to form end nose, although maneuver This generally performed if more conservative techniques are not beneficial. 15
Graft edge alarm : Graft onlay small placed to in pocket in throughout caudal aspect from incision marginal For create bulge Which tall in throughout alar margin And prevent retraction alarm. Graft edge alarm Also increase long And width of the nostrils, thereby improving the function of the external valve. 11
Alar base reduction: Limited skin in the area between the nasal sill and the ala is excised to produce the desired nostril size and base width. Alar base reduction is usually necessary when reduction of the tip projection creates a widened alar base appearance. 11
The nasal tip is anatomically formed by the ala, tip, columella , footplate, sill, soft triangle, rim, and alar sulcus. These three anatomical structures do not contain cartilage or bone tissue, only skin and soft tissue. Alar excision was first reported by Weir. Technique excision Which used since moment That has experienced a lot progress area like quality And used wound Which hidden. Excision alarm is done for the following reasons:
Narrowing down base alarm
Rotate style to on and/or to lower
Repair asymmetry alarm
Adapt size nostril
Adapt point adhesion nasolabial sulcus
Repair case lips chippy And nose
In all condition This, excision base alarm must designed primarily for individual patients.
Categorize orientation alarm wing become
Type A: Divergent
Type B: Straight
Type C: Convergence (acute)
Type B considered most aesthetic in between types other. Medialization nostrils, or narrowing of the base, is only recommended for Type A. Interventions should be performed for alar base line narration can result in Type C, which is another base anomaly if the soft tissue balance is not adjusted or if the sutures are not sewn properly.
Figure 31. Alar base surgery steps , marking the surgical site on the alar (A), done incision on threshold hole nose (B), Elevation flap (C), flap elevation and disconnection (D), suturing (E), skin suturing from median to lateral (F)
Indications for Alar Base Excision for Aesthetic Purposes. So that the appearance of the nose looks symmetrical and beautiful.
Cases where there is a wide alar base (where the alar base is wider than the intercanthal distance); the decision whether this distance is normal should be made by comparing it with the horizontal length of the eye.
A case where the alar wing is outside the inter-canthal distance despite the fact that the alar based (base of adhesion of the alar wing ) is inside.
Figure: If the nostrils are large, the distance between the nostril threshold and the base of the nostril is nose generally long. The goal is For narrow down area This
Incision: The incision should follow the nostril threshold. The nostril threshold has an anatomy that rests on the lips.
Elevate the flap and decide where to place it by pulling it with pliers.
Grab the end of the cover with pliers and stretch it. Next, place it on the base and hold it there, removing the excess.
Put it down stitches key in end closing. Repeat process in side contralateral.
Place two subcutaneous 6/0 Monocryl sutures. Close the skin from medial to lateral with a 6/0 round Prolene needle using a continuous suture technique.
Osteotomy: Precise bone cutting aims to (1) close deformities. open book (caused by by hump nose Which has cut previously) and (2) straighten out bone nose Which experience deviation as well as (3) narrowing the width of the dorsum and sidewall bones. This can be done with a combination of various osteotomy techniques (eg, medial, intermediate, and lateral) based on the existing bone deformity and the desired results. 11,16
Nasal dorsum: Dorsum modifications are best visualized and appropriately modified with an open approach. In noses with a prominent dorsum, required reduction cartilage with excision direct. On nose with projection corner nasofrontal Which No adequate, graft onlay dorsal can installed and protected using a conchal, rib, or calvarial graft. 11
Nasal Dorsum Reconstruction by performing the separation and use of cartilage back nose with spreader graft First time published by Gürsel Turgut et al. It has been mentioned previously that, in the normal keystone area , both sides bone dosrum own curve. Line aesthetics back nose until 3-4 mm above the keystone area is made of cartilage. The same anatomy will be replicated. After bone Which deviation lifted, will formed edge bone on part antero-caudal bone. The bone edges may even curve medially due to bone topograft. In patients with extreme curvature, this may prevent closure. roof. In anatomy normal, edge bone This No There is. There is bone curve in second side area keystone, And curve This containing cartilage, cut edge part bone with scissors bone. Triangle bone Which will removed measuring approximately 3 × 3 × 5 mm. If the angle is not removed, the bone becomes more dominant on line aesthetics dorsal. Handling bone more difficult. More logical to imitate anatomy the original. On case This done with use graft wing Libra into the notch formed by removing the corner of the bone. On the cartilage fusiform back nose enter to in notch bone. If want to make
spreader flap, this bone triangle does not need to be removed. However, if you want to make a Libra spreader graft , you have to remove the edge of the bone.
Closure: A septal splint (eg, trimmed silicone sheet ) may be sutured to the surgical site, although this is optional. The transcolumellar incision is then closed. with stitches permanent interrupt with use nylon 6-0 or 7- 0 or using fast-absorbing sutures , which further provides aesthetic results. similar without discomfort Which related with release stitches. The marginal incision is closed with interrupted sutures using absorbable thread (5-0 fast). 11
Taping and casting : Adhesive tape is applied from the nasofrontal angle to the supratip to help reduce postoperative edema. A longer strip is placed around the infratip lobule , serving to support the nasal tip at the desired degree of rotation. A nasal cast is then applied with a thermoplastic splint that becomes pliable when exposed to hot water and hardens when cold. Antibiotic ointment is applied to both nostrils, after which a dressing is applied . Nasal packing is usually avoided in cases of excessive bleeding. 2
2.10 Complications
Complications Which most general happen on septorhinoplasty is excessive bleeding which can usually be managed with nasal packing and may require cauterization in rare cases. Septal hematoma can happen when bleeding happen in lower mucoperichondrium, And matter This requires drainage or aspiration to prevent the development of infection, septal perforation and/or saddle nose deformity . Septal perforation can also occur due to bilateral laceration of the opposing mucosa during surgery; if the perforation approaches the keystone area, a saddle nose deformity may occur, possibly requiring revision surgery. Aesthetic complications related to cartilage weakness consequence resection excessive on septorhinoplasty like saddle nose , nasal Widening of the base , loss of nasal tip projection or dislocation may also occur. 6
Infection, nasal congestion, and prolonged healing may occur. part patient. Infection seldom happen And generally can cured with oral antibiotics. Most patients will recover completely within a few weeks. Hyposmia Also reported on a number of patient And usually disappear in six months. Intranasal adhesions can occur, but the use of silastic splints minimizes the risk of this complication. Patients may also experience numbness or increased sensitivity in the upper teeth or lip area due to manipulation of the nasopalatine nerve during surgery; this is usually short-lived, and normal sensation returns within a few months. 6,17
Some rare but life-threatening complications include skull base/intracranial injuries including traumatic cerebrospinal fluid (CSF) rhinorrhea , meningitis, pneumoencephalus, subarachnoid hemorrhage, subdural abscess, brain, thrombosis sine cavernous, And syndrome shock toxic. Giving Counseling patients about the risks that may occur before undergoing surgery is very important .
Maintenance Post Septorhinoplasty
Patients who have undergone septorhinoplasty are then sent to the recovery room for one day with the head elevated, ice compresses, and given analgesia. 11
A literature review by Kullar et al. showed that perioperative and postoperative antibiotics did not reduce the risk of infection in patients undergoing non-complex rhinoplasty or septorhinoplasty. Based on the review, when patients do have an increased risk of infection (e.g., if there is comorbidity, revision surgery, prolonged surgery, use of alloplastic implants, or use of nasal packing), physicians should consider first-generation cephalosporin antibiotics, such as cefazolin (or, in patients with β-lactam allergy, non-β-lactam antibiotics, such as clindamycin). The researchers also stated that when used on time perioperative, therapy antibiotics must started in time 1 O'clock after incision and ends within 24 hours post-operatively, unless the patient requires treatment Which prolonged. 18 Spray oxymetazoline And Saline may also be administered to provide a clean intranasal environment during the process. healing. Patient need checked in 1 until 2 Sunday For Post-operative assessment and removal of splints if used. Then follow-up is performed after 1 month post-operatively. 11
SUMMARY
Septorinoplasty is a term used when rhinoplasty and septoplasty procedures are performed simultaneously. This procedure involves surgery of the bones and cartilage in the nose to improve the shape and structure of the nose (rhinoplasty) and straighten the septum (septoplasty). 2 The indications for this operation vary widely, ranging from functional obstruction of the nasal cavity to cosmetic reasons. including cartilage alarm or cartilage lateral on Which asymmetry, end inadequate nasal support, rotation or projection, excessive nasal projection, asymmetry or deformity of the nasal tip, crooked nose , saddle nose , cleft lip or other congenital abnormalities, septal perforation and revision rhinoplasty.
REFERENCE
Sorta-Bilajac I, Muzur A. 2007. The nose between ethics and aesthetics: sushruta's legacy. Otolaryngology–head and neck surgery: official journal of the American Academy of Otolaryngology-Head and Neck. Surgery 137(5):707– 710
Ishii, LE, Tollefson, TT, Basura, GJ, Rosenfeld, RM, Abramson, PJ, Chaiet, SR, Nnacheta, LC American Academy of Otolaryngology-Head and Neck Surgery Foundation. 2017. Clinical Practice Guidelines: Improving Nasal Form and Function after Rhinoplasty. Otolaryngology-Head and Neck Surgery, 156(2S), S1-S30.
Oneal RM, Beil RJ Jr., Schlesinger J. 1996. Surgical anatomy of the nose. Clin Plast Surg 23(2):195–222
Bakshi J, Patro SK. Septorhinoplasty: Our Experience. Indian J Otolaryngol Head Neck Surg. 2017 Sep;69(3):385-391. doi: 10.1007/s12070-017-1127-0. Epub 2017 Apr 10. PMID: 28929073; PMCID: PMC5581764.
Al Arfaj A. A Rare Complication of Septorhinoplasty. Plastic Reconstruction Heaven Globe Open. 2015 Jan 8;2(12):e273. doi: 10.1097/GOX.0000000000000224. PMID: 25587507; PMCID: PMC4292255.
Watters C, Brar S, Yapa S. Septoplasty. Updated 2022 Nov 8. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023 Jan
Simon PE, Lam K, Sidle D, Tan B.K. The Nasal Keystone Region: An Anatomical Study. JAMA Facial Plast Surg. 2013 May;15(3):235-7.
Berghaus, A. 2014. Rhinoplasty: Aesthetic plastic surgery of the nose. Tuttlingen, Germany: Endo-Press.
Guyuron B, Afrooz PN. Correction of Cocaine-Related Nasal Defects. Plast Reconstr Surg. 2008 March; 121(3):1015-1023.
Most SP, Rudy SF. Septoplasty: Basic and Advanced Techniques. Facial Plast Surg Clin North Am. 2017 May;25(2):161-169.
Raggio BS, Asaria J. Open Rhinoplasty. [Updated 2023 Jul 3]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023 Jan
Aiach G. Atlas of Rhinoplasty: Open and Endonasal Approaches, Second Edition. Plast Reconstr Surg. 2005 May. 115(6):1778-9.
Fettman N, Sanford T, Sindwani R. Surgical Management of the Deviated Septum: Techniques in Septoplasty. Otolaryngol Clin North Am. 2009 Apr;42(2):241-52, viii.
Heppt W, Gubisch W. Septal Surgery in Rhinoplasty. Facial Plast Surg. 2011 Apr;27(2):167-78.
Toriumi DM, Checcone MA. New Concepts in Nasal Tip Contouring. Facial Plast Surg Clin North Am. 2009 Feb;17(1):55-90, vi.
Azizzadeh B, Reilly M. Dorsal Hump Reduction and Osteotomies. Clin Plast Surg. 2016 Jan;43(1):47-58.
Dąbrowska-Bień J, Skarżyński PH, Gwizdalska I, Łazęcka K, Skarżyński H. Complications in Septoplasty Based on A Large Group of 5639 Patients. Eur Arch Otorhinolaryngol. 2018 Jul;275(7):1789-1794.
Kullar R, Frisenda J, Nassif PS. The More the Merrier? Should Antibiotics be Used for Rhinoplasty and Septorhinoplasty?-A Review. Plastic Reconstruction Heaven Global Open . 2018 Oct. 6 (10):e1972.]
The Witch, B. (nd). Aesthetic Septorhinoplasty Second Edition .
Jankowski, R., Gallet, P., Nguyen, D.T., & Rumeau, C. (2021). Septorhinoplasty by disarticulation. European Annals of Otorhinolaryngology, Head and Neck Diseases , 138 (3), 195–199. https://doi.org/10.1016/j.anorl.2020.06.018
Kridel, R. W. H., Scott, B. A., & Foda, H. M. T. (nd). The Tongue-in-Groove Technique in Septorhinoplasty A 10-Year Experience .
Comments