SUDDEN SENSORINEURAL DEAFNESS ON MENINGITIS SUIS
I Made Nudi Arthana
Sudden sensorineural deafness is often also called sudden deafness or sudden sensorineural hearing loss, which is a type of sensorineural hearing loss. Meningitis suis caused by Streptococcus suis is one of the most common etiologies Lost of deaf sensorineural sudden on person mature. 1,2,3,4,5,6
LITERATUR REVIEW
Anatomy ear And physiology hearing
Ear divided on outer ear, ear middle And ear in. Ear The outer ear consists of the auricle and the external acoustic canal. The middle ear consists of the tympanic membrane, malleus, incus, stapes, and tympanic muscles. tensor timpani and the stapedius muscle. There is a chorda tympani which is a branch of the facial nerve that runs across the cavity The middle ear carries taste fibers. The Eustachian tube connects the middle ear cavity to the pharynx which will be opened by contraction of the tensor veli palatini muscle. 7
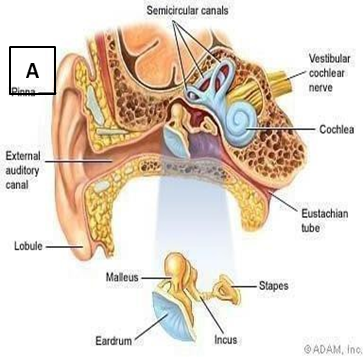
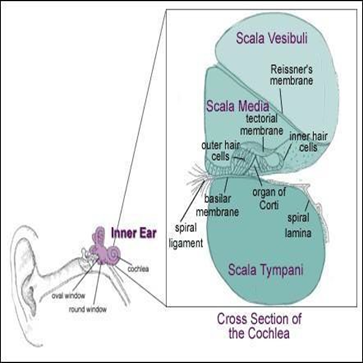
Picture 1. A. Picture schematic ear, B. Cross section transverse cochlea 7
The inner ear consists of the cochlea and the vestibular organs which are located in bone temporal. Cochlea is tube Which contain sensory organ for hearing. The cochlea has three fluid-filled canals, namely the vestibuli scale, the tympani scale and the media scale. The media is at in cochleapart middle, separated from scale vestibuli by Reissner's membrane and from the scala tympani by the basilar membrane. The scala vestibuli and scala tympani contain perilymph fluid while the scala media contains endolymph fluid. 7
The perilymph fluid in the inner ear communicates with the cerebrospinal fluid in the cranial cavity via the cochlear aqueduct, which connects room perilymph with room fluid cranial. Membrane Reisner has very high compliance so that even very small pressure changes can cause large volume changes in the endolymph space. Disturbances in the pressure balance in both systems will cause hearing and balance disorders. 1.7
The organ of Corti is located on the basilar membrane and contains many cells. sensory, outer hair cells and inner hair cells. Between the rows of outer hair cells and inner hair cells is a Corti tract. Outer hair cells are cylindrical while inner hair cells are shaped like pumpkin. Cell hair outside atapeks The cochlea is longer than the basal part. The stereocilia of the inner hair cells at the basal part of the cochlea are shorter than those at the apex cochlea. vascular striae be in between room perilymph and endolymph along the cochlear wall. The stria vascularis contains many blood vessels and mitochondria in its cells, indicating the involvement of metabolic activity. 7
The basilar membrane is about 150 μm long at the base of the cochlea and 450 μm wide at the apex, contains connective tissue and forms the basal scala media. At the basal part, the basilar membrane has a more rigid structure. compared to the apex. This gradual change in structure causes the sound reaching the ear to produce a waves on the membrane walking basilar from basal to the apex of the cochlea. 7
The cochlea is innervated by auditory afferent, efferent and autonomic nerve fibers. The cochlea is supplied by the labyrinthine artery which originates from the cerebral artery. inferior anterior cerebellum and follows the VIII cranial nerve in the internal acoustic meatus. The labyrinthine artery is the terminal artery And onlycontains A little even No There is supply collateral blood vessels to the cochlea. 7 The hearing process begins with the capture of sound energy by the cochlea. ear in the form of waves that are transmitted through the air or cochlea. After entering the meatus external, sound will thrilling tympanic membrane furthermore transmitted through the auditory ossicles. The auditory ossicles will amplify the vibrations through the leverage of the auditory ossicles and the multiplication of the area ratio of the tympanic membrane and the oval window. This amplified vibration energy will be transmitted to the stapes which will move oval window so that the perilymph in the scala vestibuli moves. Movement is continued through the pushing Reissner membrane endolymph, so that will cause motion relatively between the basilar membrane and the tectorial membrane. This process is a stimulus Mechanic Which cause the occurrence stereociliary deflection hair cells , so that the ion channels open and there is a release of electrically charged ions from the cell body. This condition will cause depolarization of the hair cells, thus releasing neurotransmitters into the synapse which will generates action potentials in the auditory nerve to to the auditory cortex in area 39-40 in the temporal lobe. 7
Deaf sensorineural sudden consequence meningitis suis
Definition And Frequency
Sudden sensorineural deafness is defined as sensorineural deafness at one or second ear that occurs rapidly within a 72-hour period with audiometric criteria in the form of hearing loss of > 30 dB at least at consecutive audiometric frequencies. deaf incident sensorineural sudden found on 5-20 per 100,000 people per year with 4000 new cases each year. 2 The distribution of male and female sufferers is almost the same. Sudden sensorineural deafness can be found in all age groups, generally in the age range of 40-50 years, with a peak incidence in the sixth decade. 2,3
Etiology And Pathogenesis
Reason deaf sensorineural suddenly arrived At the moment Not yet can be known definitely. Reported etiology from Sudden deafness can only be confirmed in 10% of these cases. The causes of sudden sensorineural deafness can be seen in table 1.
Table 1. Reason deaf sudden sensorineural 8
Reason Deaf Sensorineural Sudden | |
Cochlea | Inflammation ( Virus,bacteria, spirochetes) |
Trauma | |
Vascular | |
Hematology (anemia, embolism, disturbance coagulation | |
Disturbance connective tissue | |
Hydrop endolymph ( Meniere's disease) | |
Disturbance metabolic | |
Ototoxicity | |
Retrocochlea and the nervous system center | Meningitis |
Multiple sclerosis | |
Sarcoidosis | |
Friedreich's ataxia | |
Amyotrophic lateral sclerosis | |
Syndrome Vogt Konayagi Harada | |
Xeroderma Pigmetosum | |
Tumor (neuroma Acoustic) | |
Idiopathic | |
Meningitis suis is an inflammation of the meninges that affects the pia mater layer and the subarachnoid space including the cerebrospinal fluid. caused by infection with the bacteria Streptococcus suis which spreads into the blood and moves to the brain fluid. 4 Streptococcus suis is pathogenic in pigs and can cause severe systemic infections in humans. Streptococcus Suis has been reported First time on year 1954 after happen meningitis, sepsis and arthritis purulen on piglets by doctor animal. Fourteen years later the first human cases were reported in Denmark and then in other places also found in Hong Kong and Northern Europe. 6 Amount case in humans infected S. Suis Keep going increased on the following year. At the end of 2012, 1584 cases of human S. Suis infection were reported . Where most cases were found most in Thailand, Vietnam And China. Besides on pig, S. Suis can also isolated from animal other like cat, dog, deer And horse And is germs commensal on intestines fine. Pig Healthy can carry multiple serotypes of S. Suis in the nose, tonsils, upper respiratory tract, genital tract and gastrointestinal tract. Of the 35 serotypes only a few cause infection in pigs that is serotype 1-9 And 14. S. Suis Serotype 2 is the most pathogenic serotype in humans and pigs. 6,13
Since the first case of S. Suis in Denmark was reported, cases have increased in several countries. 151 cases of Suis meningitis were reported. in Vietnamese in period 10 year. 13 Sporadic cases of infection have also been reported where infection S. Suis in province Sichuan China during July and August as many as 215 cases and 38 cases caused death. The cases emphasize S.Suis infection as dangerous zoonotic disease . S. Suis serotype 2 is the most common cause in humans. 13 Infections S. Suis in humans has been reported in countries with high pork consumption. The highest incidence happen on group age 47-55 year And seldom happen in children. Ratio incident on man and woman that is 3.5 : 1 until 6.5 :
1 that supports the occurrence of occupational infections. Farmers and workers who deal with pigs have the highest risk. caught meningitis suis Where reported happen 3 case per
100,000 population, the risk is lower in butchers where there are 1.2 cases per 100,000 population in developed countries. But the incidence is not in accordance in southeast asia where the population high pigsSome theories of the occurrence of idiopathic sudden sensorineural deafness are damage to the vestibulocochlear nerve by a viral infection, vascular disorders, or rupture of the labyrinthine membrane. Suspected causes of idiopathic sudden deafness include infection virus, immunological, abnormality vascular And rupture membrane intracochlear but none of them can explain with certainty the pathophysiological process of idiopathic sudden deafness. 8
Infection virus allegedly as Wrong One reason deaf sudden sensorineural deafness. Wilson presented data with seroconversion examination of the virus in patients with sudden sensorineural deafness, most of whom were sensorineural deafness sudden due to by virus Herpes. Inspection serological studies of patients with idiopathic sudden sensorineural deafness showed increased antibody titers against a number of virus. Histopathological examination temporal bone in sensorineural deafness patients suddenly this found cochlear damage due to injury from the infection, loss of hair cells and supporting cells, atrophy of the tectorial membrane, atrophy of the stria vascularis. 8,9
The vascular disorder theory is the most widely developed theory. The cochlear blood vessels are end arteries with circulation. who does not collateral And its function in a way smooth to change the blood supply so If there is a disturbance in these blood vessels, the cochlea is very easily damaged and ischemia occurs. This blood vessel disorder can be caused by embolism, thrombosis, lack of blood flow, vasospasm and hypercoagulation or increased viscosity. Ischemia results in degeneration wide in the ganglion cells of the stria vascularis and spiral ligaments. Then followed by the formation of connective tissue and reinforcement. 8.9
In the theory of intracochlear membrane damage, it is said that there is a thin membrane that separates the inner ear from the middle ear and there is a fine membrane that separates the perilymph space from the endolymph in the cochlea. A tear in one or both of these membranes theoretically can cause deaf sensorineural. Leakage fluid Perilymph into the middle ear through the round window and oval window is postulated to cause deafness by forming relative endolymph hydrops or causing a tear in the intracochlear membrane. A tear in the intracochlear membrane allows the mixing of perilymph and endolymph, thus changing the endocochlear potential. 8,9
Sensorineural deafness caused by autoimmune processes is introduced by McCabe on year 1979. 1 On condition This progressive hearing loss was found. There is immune activity in the cochlea support draft theory This. Disturbance hearing on Cogan's syndrome , SLE And abnormality autoimmune rheumatism other has long known. 3 As Supporter other theory This, there is A studies prospective on 51
patients with sudden sensorineural deafness and several abnormalities related to the immune system ( multiple immune-mediated disorders ) were found. 8 In research in Sinhuan Province, China risk of infection S. Suis occurs in people who cut and process pork as well as on for breeder pig. Consuming meat pig Which Undercooked food is also a risk factor for human S. suis infection. It is still a matter of debate how S. suis invades the host and how it can cross the blood-brain barrier. A series of potential virulence factors of S. suis serotype 2 have been identified, including capsular polysaccharide, extracellular protein factors, released-muramidase protein, suilysin, adhesins, hyaluronate lyase, and surface antigen 1. Except for the capsular polysaccharide, none of these factors have been proven to be important for the virulence of S. Suis . 14 Infection can reach the meninges through the bloodstream (hematogenous) due to infections elsewhere such as pharyngitis, tonsillitis, endocarditis, pneumonia, infection. S. Suis meningitis mostly occurs due to hematogenous spread through the process of bacteria adhering to the epithelial cells of the mucosal port of entry , penetrating the mucosal barrier and multiplying in the bloodstream and causing bacteremia. Bacteremia can continue into the cerebrospinal fluid (passing the blood-brain barrier) and multiplying in the cerebrospinal fluid, causing inflammation on membrane brain ( meninges ) And brain. 13.15 There is Several hypotheses regarding the route of entry of the bacteria causing meningitis to the cochlea. The first route is through the bloodstream. This hypothesis is said to be very reasonable because S. suis infection begins with bacteremia. on phase I. Matter second Which support hypothesis These are the spiral structures of the limbus and the lateral wall of the cochlea consisting of the stria vascularis and the spiral ligament are structures with high vascularization. 2.6 The next supporting reason is the finding of granulocytes in the spiral ligament. 7 However, there are several reasons against hypothesis This. In a number of studies No found infection on a scale media, whereas inflammation happen in scale timpani. Limbus spiral just bordering with scale vestibule And location lateral wall The cochlea generally faces the scala media. This could explain the inflammation in media scale not as bad in scale timpani is high potassium content in endolymph. An environment with high potassium levels can be an unfavorable environment for bacteria and granulocytes, which may explain the lack of inflammation in scale media.10 Hypothesis second about route infection bacteria causes of meningitis into The cochlea is via the 8th cranial nerve (vestibulocochlear nerve). There are several reports of severe meningitis cases that have evidence of inflammation along the cochlear nerve. 10 However, not all cases have suppurative labyrinthitis. and some patients with suppurative labyrinthitis no inflammatory cells in the modiolus. 10 Involvement of the retrocochlear structures is very rare and inflammatory cells are usually not found along the neural network in animal models of meningitis. 28 The third hypothesis is the spread of infection through the cochlear aqueduct or perilymphatic duct. The perilymphatic duct connects the subarachnoid space to the posterior cranial fossa with the basal turn of the scala tympani. The perilymphatic duct structure is filled with soft connective tissue, but there is still enough space for fluid, erythrocytes, and bacteria to pass through. 7 S. suis bacteria enter through the cochlear aqueduct into the perilymph and cause nerve damage due to exotoxin. The cochlear aqueduct connecting the subarachnoid space to the basal turn of the scala tympani is a location indicated as an intermediary for the occurrence of meningogenic labyrinthitis. 10 This can be used For explain Why colony bacteria And concentration inflammatory cells tall in basal turn from scale timpani. 20 Besides That, ossification also more often happen in location Which The same. So that, can explained that high frequency hearing loss associated with the basal turn of the cochlea is more common than low frequency hearing loss associated with the apex region of the cochlea. Cochlear aqueduct Which short And patent on child cause existence the tendency for sensorineural deafness associated with meningitis is more common in patient child compared to adult. 10 Advanced from infection meningeal and/or inflammatory processes from the subarachnoid space through the cochlear aqueduct and/or internal auditory canal into the inner ear cause labyrinthitis and consequent lesions. on the target organ. This process will lead to deafness. In general, external pathogens such as components from cell bacteria cytotoxic will stimulate release proinflammatory cytokines including Tumor Necrosis Factor-α (TNF-α) and Interleukin-1 (IL-1). Inflammatory responses will be induced and eventually cause damage to the cochlea. Byproducts of inflammation such as Nitric Oxide (NO), superoxide and peroxynitrite contribute to the damage. BLB and induce cytotoxic effect on hair cells and SGN. [29] Other deficits include cochlear ischemia following septic embolism and thrombotic occlusion of small blood vessels supplying the inner ear and neuronal damage following neuritis or hypoxia. 10
Diagnosis
The diagnosis of sudden sensorineural deafness is based on anamnesis, physical and ENT examinations, pure tone audiometry, and other supporting examinations. In the anamnesis, the patient's complaint is a sudden hearing loss, within a few hours or days, in one or both ears. In addition, it can also be accompanied by complaints of tinnitus and peripheral vestibular vertigo. Medical history previous need asked especially the disease can become risk factors as well as a history of use of ototoxic drugs. 1.8 In the ENT examination, no abnormalities were found in the ear canal. acoustician external And membrane timpani. Through inspection The Rinne test results were positive, Weber lateralized towards the affected ear. healthy and Schwab shorten. On inspection audiometry pure tone mild sensorineural deafness was found to severe, either at low, medium, high or all frequencies. 3.8 Inspection Auditory Brainstorm Response (ABR) used For to rule out lesions in the cerebellopontine angle (CPA) or internal auditory canal (IAC) as the cause of unilateral deafness. ABR is particularly useful when MRI is unavailable or contraindicated. MRI. Sensitivity inspection ABR For diagnose lower tumor compared to with MRI, namely 88% compared to with 99%. However, in tumors that are large in size
Inspection laboratory done based on history disease and suspected diagnosis such as complete blood count, blood sugar, lipid profile, hemostasis function, chest X-ray, and electrocardiography. 3.8
The diagnosis of Suis meningitis is made through anamnesis, examination physique And inspection support. On anamnesis complaints received meningitis in the form of fever tall (94%), painful head great, nausea, vomiting (82%), diarrhea, stiff neck, decreased consciousness, seizures and abnormalities focal neurology. As well as on meningitis Suis reported more of 50% of cases there is a sensorineural type of hearing loss. Hearing loss in Suis meningitis is a sensorineural type, at high frequencies, can be profound where hearing loss reaches more than 80 dB on audiometry examination. 4,6
On physical examination, a decrease in consciousness may be found. can be assessed with Glaslow Coma Scale. There is also signs of meningeal irritation which can be checked with several parameters including other checks rigid neck, sign Kernig, sign Brudzinski I and Brudzinski II. 13
Supporting examinations carried out are by blood culture or from cerebrospinal fluid through lumbar puncture using standard microbiology technology to identify Streptococcus suis and its serotypes. Identification of Streptococcus Suis can also be done if the culture results are doubtful, namely with specific molecular techniques with PCR Serotype Suis serotype 2. 14,15
Management deaf sensorineural sudden consequence meningitis Suis
Management of sudden sensorineural deafness should be based on the cause, however, because most cases of sensorineural deafness sudden is idiopathic so that treatment done empirically. 1,3,4
Several studies of corticosteroid use in patients with sudden deafness have been published. There is laboratory evidence that suggests an inflammatory cascade of cell death in patients with sudden deafness that is modified by steroid therapy. Corticosteroids given are oral, intravenous and/or intratympanic synthetic glucocorticoids, including prednisone, methylprednisolone, and dexamethasone. Corticosteroids are thought to have effect anti-inflammatory And ability to increase cochlear blood flow. For maximum treatment results, the recommended dose of oral prednisone therapy is
1 mg/kg/day single dose with a maximum dose of 60 mg/day for 10-14 days. The equivalent dose of 60 mg prednisone is equivalent to 48 mg methylprednisolone and 10 mg dexamethasone. 3 A representative data use regimen treatment with dose maximum for 4 days followed by tapering off 10 mg every two days. 3.8
Some otolaryngologists recommend intratympanic corticosteroid therapy as an alternative to systemic corticosteroid therapy or “ salvage therapy ” in patients who do not improve with systemic corticosteroids. The advantage of intratympanic corticosteroid therapy is that it delivers high concentrations of steroids directly to the target tissue (perilymph) with minimal systemic side effects. 5 This is supported by Parnes et al., who published and demonstrated high steroid levels in the inner ear after intratympanic steroid therapy application. A study of the combination therapy of high-dose systemic corticosteroids and intratympanic corticosteroids showed results in significant improvement in hearing function. 10 The intratympanic steroid commonly given is dexamethasone. or methylprednisolone. Concentration corticosteroids Which used varies, most studies recommend dexamethasone 10-24 mg/mL and methylprednisolone 30 mg/mL or more. 5,10,12
Hyperbaric oxygen therapy as an additional therapy in cases of sudden deafness. This therapy provides 100% oxygen with a pressure of more than 1 ATA ( atmosphere absolute ). This therapy aims to increase cochlear and perilymph oxygenation, so it is expected to be able to to deliver oxygen with pressure partial Which more tall to the tissue, especially the cochlea which is very sensitive to ischemic conditions. Hyperbaric oxygen therapy is thought to have complex effects on the body's immunity, oxygen transport and hemodynamics, increasing normal host response to infection and ischemia, and reduce hypoxia and edema. 10 According to the AAO-HNS guidelines , oxygen therapy Hyperbaric should be done in 2 weeks to 3 months from moment diagnosis deaf sudden. Patient age young give better response compared to more patients old (age varies) between 50-60 years). important things to consider in therapy hyperbaric oxygen This is benefit And risk effect side. Therapy This has side effects in the form of damage to the ears, sinuses and lungs due to changes pressure, myopia Which getting worse temporary, claustrophobia, and poisoning oxygen. 11
In addition to viral infections, other causes of sudden deafness are cochlear ischemia due to vascular disorders, such as hemorrhage, embolism, and vasospasm. Vasoactive agents, thrombolytics, vasodilators or antioxidants have been tried to increase cochlear blood flow, but there is no evidence of therapeutic success. Ginkgo biloba extract containing flavones and terpenes can prevent the development of free radicals and act as a vasodilator. Pentoxifylline inhibits platelet aggregation and increases the flexibility of erythrocytes and leukocytes, thereby improving viscosity blood, especially vessels capillary. Dextran can improve microcirculation because it has antithrombotic effects. HES ( hydroxyethylstarch ) reduces hematocrit and platelet aggregation. 10,11
As with other bacterial meningitis management, broad-spectrum antibiotics may be given pending culture and antibiotic sensitivity results. Data from previous studies are still sensitive to penicillin, ceftriaxone And vancomycin. Antibiotics that are resistant to erythromycin, tetracycline, and chloramphenicol can be given for 14 days at LPS evaluation on day 13. . 6
The use of dexamethasone as an adjunct treatment to reduce mortality and improve outcomes of bacterial meningitis is controversial. In a study in Vietnam, dexamethasone administration significantly reduced the risk of death and disability. In another multivariate analysis, significant results were obtained where cases of severe hearing loss in patients over 50 years occurred when corticosteroids were not given. 6,16
Prognosis
The prognosis for sudden deafness depends on several factors, namely age, degree of impairment. hearing, method treatment Which used, when starting treatment, the presence or absence of vestibular symptoms and predisposing factors other. Age carry on, disturbance hearing very severe and there are symptoms subjective vestibular dysfunction is associated with a low recovery rate. 11 Advanced age, hypertension, diabetes, and hyperlipidemia are associated with microvascular dysfunction in the cochlea, which is a poor prognostic factor. Early initiation of treatment is associated with a good prognosis for hearing recovery. The degree of initial hearing loss affects the potential for hearing recovery. Vertigo can be used as an indicator of lesion severity and is associated with a poor prognosis. 11,12 However, 28-65% of untreated sudden deafness patients can experience spontaneous recovery. Patients with sudden deafness who have received treatment but the deafness remains permanent and causes disability, requiring auditory rehabilitation. 8 The prognosis of Meningitis suis is good, where it is rarely reported to cause death compared to with meningitis bacteria Which due to types of bacteria other like Streptococcus pneumoniae
The success of treatment for sudden sensorineural deafness is assessed based on the average hearing threshold according to Siegel, namely a) Total recovery if the average hearing threshold is < 25 dB, b) Recovered partially if there is improvement > 15 dB with an average hearing threshold of 25-45 dB, c) mild recovery If repair > 15 dB withthreshold hear average > 45 dB, d) no There is recovery If repair < 15 dB. 12 Complications consequence infection
S. suis more often reported compared to reason other with sensorineural deafness as the most frequent complication
CONCLUSION
A case of sudden severe right sensorineural deafness has been reported. and hereafter et cause meningitis suis , on man age 49 year
, Balinese Tribe. The patient has a hobby of consuming pork lawar, especially red lawar. The patient was treated with medication with the results determined based on the degree of deafness in the first audiogram, type of audiogram, onset of predisposing factors.
Sudden sensorineural deafness is an emergency case. which requires Handling immediately. Meningitis Suis is meningitis caused by Streptococcus suis infection which is acquired through exposure to contaminated pork or contaminated pork. Reported more from 50% patient with Meningitis Suis has complaints of hearing loss. If the diagnosis and treatment are late, it will cause permanent deafness. Pathogenesis of sudden hearing loss in Meningitis suis Still Not yet known with clear. Meningitis disease suis that can be treated because still sensitive to antibiotics and the prognosis is good. Prevention can be done by reducing contact direct with pig with use protective equipment and process the pork until it is perfectly cooked.
REFERENCE
Hashisaki. Sudden Sensory Hearing Loss. In Bailey's: Otolaryngology Head and Neck Surgery. 5th edition. Philadelphia. Lippincott Williams and Wilkins. 2014; p.2589-94.
Levie, P., Desgain, O., Burbure, C. Sudden Hearing Loss. B-ENT Supplement6. 2007; 3: 33-43.
Hidayat, H, Edward, Y., Hilbertina, N., Description of Sudden Deafness Patients in the ENT-KL Department of Dr. M. Djamil Padang General Hospital. Andalas Health Journal. 2016; 5(2)
Hey JH, Kyoun JP et a. Streptococcus suis Meningitis with Bilateral Sensorineural Hearing Loss, Korean J Lab Med, 2011; 31: 205-211
Feng Y, Zhang H et al. Streptococcus suis : an emerging/reemerging challenges of bacterial infectious diseases, Virulence. 2014; 5:4: 477-97
Plaza G, Durio E, Herraiz C, Rivera T, Garcia-Berrocal JR. Consensus on diagnosis and treatment of sudden hearing loss. Ata Otorrinolaingol Esp. 2011;62(2):144-57
Weber PC, Khariwala S. Anatomy and Physiology of Hearing. In: Johnson JT, Rosen CA, editors. Bailey's Head and Neck Surgery Otolaryngology. Otology 2. 5 ed. Philadelphia: Lippincott Williams & WJ.lKins; 2014. p.2253-73.
Kuhn M, Heman-Ackah SE, Shaikh JA, Roehm PC. Sudden Sensorineural Hearing Loss: A Reviews of Diagnosis, Treatment, and Prognosis. Amplif Trends. 2011;15(3):91-105.
Malley MR, Haynes DS. Sudden hearing loss. Otolaryngol Clin N Am. 2008;41:633-49.
Khater A, El-Anwar MW, Nofal AA, Elbahrawy AT. Sudden Sensorineural Hearing Loss: Comparative Study of Different Treatment Modalities. Int Arch Otorhinolaryngol . 2018;22(3):245 ‐ 9.
Chandrasekhar SS, Poll GL, Watch DM. Clinical Practice
Comments