VESTIBULITIS NASAL
I Made Nudi Arthana
VESTIBULITIS NASAL is inflammation of the nasal vestibule area, which is the skin-lined front part of the nostrils. This condition is generally caused by a bacterial infection, especially Staphylococcus aureus , but can also be triggered by physical or chemical irritation, as well as repeated trauma from habits such as excessive nose hair plucking or nose picking. 1-3 Small injuries to the nostrils can cause pimples at the base of the nose hairs and sometimes crusts around the nostrils. Repeated trauma to the vestibule when the nose is wiped And in clean by patient Alone become reason most often Apart from that, plucking or cutting nose hair can irritate the skin of the nasal vestibule, thereby triggering infection.
LITERATURE REVIEW
Anatomy Nose
The shape and appearance of the external nose not only affect the overall appearance, but also the functional processes that occur inside the nose. The anatomical structure of the nose is important for both aesthetic and functional reasons, because the nose is the gateway to the respiratory tract. 4
The external nose is an extension of the nasal cavity that projects toward the front of the face and positions the nares to curve downward. The external nose is pyramidal in shape with the apex in the anterior. The upper corner of the nose between the orbital bones continues to the forehead. The structure of the external nose consists of bones and cartilages and connective tissues. The bony part is the part where the nose connects to the skull, here the nasal bone and part of the maxillary bone and frontal bone also support it. In the anterior part, on each side, it is composed of the lateral processes of the septal cartilage, the major ala and three or four minor ala cartilages, and a septal cartilage in the midline that forms the anterior part of the nasal septum. 4
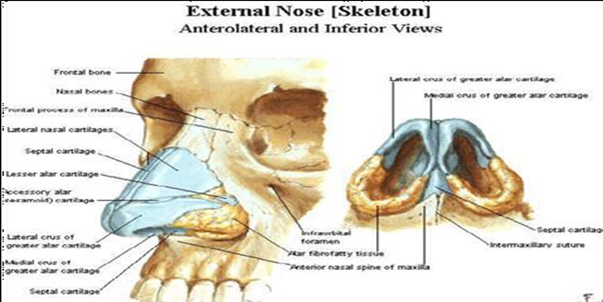
Picture 2.1 Anatomy bone nose 2
The nasal cavity is a space, where there is an entrance in the anterior part called the anterior nares while in the posterior part the boundary between the nasal cavity and the nasopharynx is called the choana. The nasal cavities are separated from each other by the nasal septum, bordering the hard palate in the inferior part, on the superior side bordering the frontal bone, ethmoid bone and sphenoid bone. On the lateral side it borders the orbit. Each nasal cavity consists of three parts, namely the nasal vestibule, respiratory area, olfactory area. The nasal vestibule is the most anterior part of the nasal cavity, which is lined with the same epithelium as the outer skin, namely stratified squamous keratinized epithelium and there are fine hairs called vibrissae. 4,5

Picture 2.2 Anatomy nose 4
Vascularization Nose
The external nose receives blood supply from the facial artery, which originates from the external carotid artery and the ophthalmic artery, which is a branch of the internal carotid artery. While the internal nose also receives blood supply from the external carotid arteries (sphenopalatine artery, greater palatine artery, superior labial artery, lateral nasal artery) and the internal carotid artery ( anterior and posterior ethmoidal). 4
The distribution of venous blood vessels in the middle part of the face is characterized by a system of interconnected and valveless venous connections between the facial and facial veins. vein angular as well as vein ophthalmic superior And sine cavernosus. Veins The face is also connected to the cavernous sinus via the inferior ophthalmic vein and the pterygoid plexus . In this pathway, infections in the skin of the middle part of the face (the so-called “dangerous” area) have the potential to spread into the brain, causing cavernous sinus thrombosis. 4,5
The nasal cavity receives a lot of blood flow from the arteries. sphenopalatine artery, which is a terminal branch of the maxillary artery in the pterygopalatine fossa. The palatine artery major give vascularization in area wall medial And floor from the nasal cavity which will anastomose with branches of the sphenopalatine artery. Vascularization of the superior labial artery for the lip area and provides branches for the nose and nasal cavity. The lateral nasal artery which is a branch of the facial artery provides blood flow to the external nose and branches alar arteries that run around the lateral edges of the nares provide blood flow to the nasal vestibule. While the anterior and posterior ethmoidal arteries, which are branches of the ophthalmic artery, provide blood flow to the medial and lateral walls of the nasal cavity, the anterior ethmoidal artery also provides blood flow to the skin and adjacent tissues of the external nose. 4
Journey vein in cavity rice part big follow arteries. Veins which follows the maxillary artery drains blood into the veins in the pterygoid plexus in the infratemporal fossa. The veins from the anterior nasal cavity join the facial vein. 4

Picture 2.3 Nasal vascularization 4
Histology
Slime Palut
The mucous membrane is a thin, sticky and tough sheet, which is a material secreted by goblet cells, seromucous glands and lacrimal glands. Consists of two layers, namely the layer that covers the ciliary shaft and microvilli ( sol layer ) which is called the periciliary layer. The periciliary fluid contains mucus glycoproteins, serum proteins, low molecular weight secretion proteins. This layer plays a very important role in ciliary movement, because most of the ciliary shafts are in this layer, while ciliary beats occur in this fluid. It is suspected that this mucoglycoprotein captures inhaled particles and is released by mucociliary movement, swallowing and sneezing. This layer also functions as protector on temperature cold, humidity low, gas or inhaled aerosols and inactivation of viruses trapped in the periciliary fluid depth are very important for regulating the interaction between cilia and mucus membranes, and are very important in determining the regulation of mucociliary transport. 6
Membrane Basalis
The basement membrane consists of a thin layer of double membrane beneath the epithelium. Beneath this double layer is a thicker layer consisting of collagen and fibrilreticulin. 5
Lamina Propia
Lamina propria is the layer under the basal membrane. This layer is divided into four parts, namely the subepithelial layer which is rich in cells, the superficial glandular layer, the media layer which contains many cavernous sinusoids and the deep glandular layer. The lamina propria consists of connective tissue, connective tissue fibers, ground substance, glands, blood vessels and nerves. The mucosa in the paranasal sinuses is a continuation of the nasal mucosa. The mucosa is thinner and has fewer glands. There are more cilia near the ostium, their movement will flow mucus towards the nose through each ostium. Among All paranasal sinuses and the maxillary sinus have a density of goblet cells maximum 5

Picture 2.4 Histology nose 6
Definition
Vestibulitis Nasal is a local infection of the hair-bearing vestibule of the nose, most commonly caused by Staphylococcus aureus. ( S. aureus ). The condition is associated with minor topical trauma such as nose picking, pulling out hair that is the entry point for infection, and long-term topical nasal steroid therapy. 1-3

Picture 2.5 Vestibulitis
Epidemiology
Although there has been no research to date on the incidence or prevalence of vestibulitis nasal , in general vestibulitis nasal is more common in older people. 1
Etiology
The cause of vestibulitis nasal is often associated with local trauma to the skin in the nasal vestibule due to frequent picking (picking). dirt nose). Cutting nasal hair can injure the skin of the nasal vestibule, causing infection. 2,7,8
Organism The cause of vestibulitis nasal is Staphylococcus aureus . Staphylococcus aureus is a gram-positive bacterium that produces yellow pigment, is facultative aerobic, does not produce spores and is not motile, generally grows in pairs or groups. This bacterium is a normal human microflora and is usually found in the upper respiratory tract and skin. Staphylococcus aureus infection is associated with several pathological conditions, including boils, acne, pneumonia, meningitis, and arthritis. Most diseases caused by this bacterium produce pus, therefore this bacterium is called pyogenic, Staphylococcus aureus also produces coagulase enzymes and catalase enzymes. 1,2
Factor Risk
Risk factors for this condition include bad habits such as nose picking, viral infections, chronic rhinorrhea, nasal hair folliculitis. And removing nose hair when suffering from a cold or flu. Other risk factors include nasal fractures from car accidents, physical fights, falls, or other traumatic causes. Septal perforation from inhaling drugs such as cocaine or methamphetamine, smoking, and exposure to toxins. In addition Conditions that affect the immune system such as systemic diseases, diabetes mellitus or in immunocompromised patients can facilitate the occurrence of vestibulitis nasal . 3,7,8
Manifestation Clinical
It starts with mild symptoms, but if manipulated by touch or squeezing movements can cause vestibulitis of the nose. The tip of the nose is felt to be very painful and stiff, where the skin is very stretched on the perichondrium. Rudolf sign is erythema on the nasal tip, more often unilateral, rarely bilateral. Additional symptoms such as fever, headache, and malaise can be found. 7,8
Vestibulitis nasal usually presents with severe pain, redness, and swelling of the nasal vestibule and tip. Physical examination reveals redness, swelling, and severe pain when the nasal tip is manipulated. Thick yellow crusts covering the nasal septum are a common finding. Systemic symptoms and signs are uncommon but may be followed by complaints of fever and increased white blood cell count. Vestibulitis nasal may be accompanied by mid-facial cellulitis and abscess formation requiring drainage. If left untreated, Vestibulitis nasal may progress to severe mid-facial cellulitis with possible associated intracranial complications. 8
Diagnosis
Diagnosis is made from anamnesis and physical examination. From anamnesis, complaints of a sore, swollen, or even feverish or malaise nose tip are usually obtained. Physical examination of Vestibulitis nasal sometimes started with the presence of furuncles, but usually they have been touched or picked at frequently, resulting in cellulitis. Other clinical findings include edema which is accompanied by redness, induration, pimples around the hair follicles of the nose, and there may even be suppuration or crusting. 8
Differential Diagnosis
Differential diagnosis of nasal Vestibulitis nasal is furuncolysis, cellulitis, rhinophyma and erysipelas. 9
Therapy
Antibiotics for vestibulitis nasal usually respond well. Treatment of vestibulitis nasal may involve topical or systemic antibiotics, especially if bacterial infection is suspected. Antibiotic ointments such as mupirocin are usually effective. 9,10 Anti-inflammatory medications should be given to reduce edema and inflammation. Cold compresses can also be used to inhibit the spread of inflammation and, no less importantly, patients are advised to always maintain nasal hygiene. 1,2,9
Although local treatment may be sufficient for mild cases, systemic antibiotics and topical treatments are indicated for more severe infections. Most cases can be treated on an outpatient basis; however, inpatient care is indicated for complicated cases, including treatment failure or the presence of cellulitis and abscesses.
To prevent vestibulitis nasal , avoid trauma to the nose such as plucking nose hairs or excessive nose picking. Managing conditions that can lower the immune system can also help prevent vestibulitis. 1,2,7-9
Complications
Complications can be very serious. They can be recognized as cellulitis, abscess and thrombophlebitis of the cavernous. The possibility of cavernous sinus thrombophlebitis should always be suspected, this can occur due to the retrograde spread of infection through the veins. This condition causes a serious condition, which is often followed by blindness or even death. Initially the patient complains of headache ,
pain to paresthesia of the trigeminal nerve followed by neuropathy of other cranial nerves, causing ophthalmoplegia. 1,2,8,9
REFERENCE
Noga Lipschitz, Arkadi Yakirevitch. Nasal vVestibulitis: etiology, risk factors and clinical characteristics A retrospective study of 188 cases, Department of Otolaryngology and Head Neck Surgery, Sheba medical center, Tel Hashomer, Israel; Elsevier 2017:131-134
Sheik-Ali, S., Sheik-Ali, S., & Sheik-Ali, A. (2022). Nasal vestibular furunculosis: Summarized case series. World journal of otorhinolaryngology - head and neck surgery , 8 (3), 217–223. https://doi.org/10.1016/j.wjorl.2020.12.003
Luan CW, Tsai MS, Liu CY, et a. Increased Risk of Nasal Septal Abscess After Septoplasty in Patients with Type 2 Diabetes Mellitus. Laryngoscope .2021;131(8):E2420-E2425. doi:10.1002/lary.29336
Bailey, BJ, Johnson .JT, and Newlands, SD, Head and Neck Surgery, Otolaryngology. Edition 4. Philadelphia: Lippincott Williams and Wilkins.2009:9:606-14
Drake RL, Vogl W, Mitchell AWM. Gray's Anatomy for Students. Philadelphia; Elsevier. 2015.67 -690
Gartner, LP, & Hiatt, J. L, 2022, Color Atlas of Histology, 8th Edition, South Tangerang, Binarupa Aksara.
Guakil, Alberto & Espinosa-Mancilla, Angélica & Olvera-Suárez, María & Anuar, Kuri Garcia. (2019). Nasal Tip Abscess: A Rare Infection of the Head and Neck. International Journal of Contemporary Medical Research.D150-D151. 10.21276/ijcmsr.2019.4.4.35.
Sil A, Panigrahi A. Rudolph Sign in Nasal Vestibular Furunculosis. October, 19th 2021. 241:258–9.
Nursanto, Dodik & Putri, Maretta & Sukirnowati, Ajeng & Fajri, Cheni. (2024). Analysis of Furuncle Management in the Nasal Vestibular. Cerdika: Indonesian Scientific Journal. 4. 825-829. 10.59141/cerdika.v4i10.2046.
Mohamed-Yassin MS, Mohamad-Isa MZ, Baharudin N. A red and swollen nose. Malaysian Fam Physician . 2020;15(1):61-63. Published 2020 Mar 18.
Comments