LITERATUR REVIEW
I Made Nudi Arthana
1. Anatomy Bone Temporal
Bone temporal consists of from pars squamous, pars timpanica, pars mastoidea, pars petrosa and stylomastoid process. Pars squamosal with fairly thin bone, convex out from the attachment point of the temporalis muscle. Pars tympanica shaped cylinder size ± 2 cm Which together pars squamous forms the external auditory canal and with the pars mastoidea forms the pars timpanica Which containing nerve vagus. Pars squamous, pars timpanica And The zygomatic process together forms the mandibular fossa. The sternocleidomastoideus, splenicus capitis, longissimus and digastricus muscles are attached to the mastoid process, while the petrous process contains the labyrinth. 3

Figure 1 Anatomy bone temporal
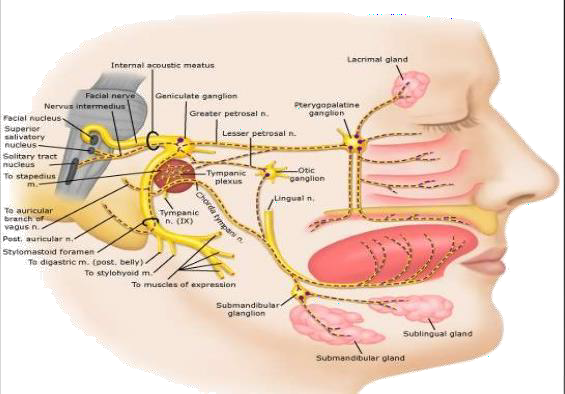
2. Anatomy Nerve Facialist
Nerve facialist consists of from 3 component that is component motorist, sensory and parasympathetic, namely: 1) motor fibers innervate the stapedius muscle, posterior venter of the digastric muscle, ear muscles and all the muscles of facial expression except muscular lifter palpebra superior, 2) fiber nerve sensory towards the taste glands of the anterior 2/3 of the tongue via the chorda tympani, 3) parasympathetic fibers towards the lacrimal glands, submaxillary glands and sublingual glands. 4.5
The anatomical unit of a facial nerve neuron consists of a cell body, an axon and a sheath. nerve. Body cell located in nucleus nerve facialist in stem brain. From The cell body projects outward forming an axon that travels through the cerebellopontine angle, temporal bone, parotid gland until it reaches the facial muscles it innervates.
Axon surrounded by sheath myelin, Which formed by cell Schwann. These cells are arranged in a connected manner and the connection area is called the Node of Renvier. Inside the axon there are neurofilaments and microtubules that function in the axon transport mechanism.
 The nerve sheath consists of 3 layers, namely epineurium, perineurium and endoneurium. Endonerium surrounds each nerve fiber, providing an endoneural tube. This tube is necessary for nerve regeneration. Thus if the endonerium is disturbed the prognosis for restoring function is worse. The perineurium surrounds a group of nerve fibers. It provides tension strength, protects the nerve from infection and provides pressure regulation. The last component is the epineurium which surrounds the entire nerve and is responsible for providing nutrition to the nerve through the vasa nervorum. 6,7
The nerve sheath consists of 3 layers, namely epineurium, perineurium and endoneurium. Endonerium surrounds each nerve fiber, providing an endoneural tube. This tube is necessary for nerve regeneration. Thus if the endonerium is disturbed the prognosis for restoring function is worse. The perineurium surrounds a group of nerve fibers. It provides tension strength, protects the nerve from infection and provides pressure regulation. The last component is the epineurium which surrounds the entire nerve and is responsible for providing nutrition to the nerve through the vasa nervorum. 6,7

Picture 2. Journey facial nerve
From both nuclei, the facial nerve fibers run around the abducens nerve nucleus, then leave the pons together with the cochleovestibular nerve and nerve intermediate Wrisberg Then enter to in bone temporal through the internal acoustic canal. In the temporal bone, the facial nerve will run in a channel bone Which called channel Fallopian. Journey nerve facialist in bone temporal shared become 3 segment, that is:

Picture 3. Chart segment, function And journey facial nerve
The labyrinthine segment is located between the end of the internal acoustic canal and the geniculate ganglion and is 2-4 mm long. The greater superior petrosal nerve exits from the geniculate ganglion and provides stimulation for secretion in the lacrimal gland.
The tympanic segment or horizontal segment, is located between the distal part of the geniculate ganglion and runs towards the posterior part of the middle ear, then up towards the oval window and stapes, then down parallel to the horizontal semicircular canal, its length is ± 12 mm. Usually the bony part of the horizontal semicircular canal protrudes laterally from the facial canal, the anterior part is 0.1-1 mm away and the posterior part is 2-3 mm away. Here the stapedius nerve exits which innervates the stapedius muscle.
Segmen mastoid or segment vertical, length 15-20 mm. Segmen This starting from the medial and posterior walls of the tympanic cavity. The transition from the tympanic segment to the mastoid segment is called the pyramidal segment or external genu. This section is the most lateral part of the facial nerve so that during surgery it is easily traumatized. The length of the pyramidal segment is approximately 2-6 mm. The wall Laterally it is the lower medial border of the aditus ad antrum . The mastoid segment runs caudally towards the stylomastoid foramen which is located in the digastric cleft. Around the middle of the mastoid segment, the facial nerve branches into the chorda tympani which carries taste fibers to the anterior 2/3 of the tongue, pain, temperature and the posterior wall of the external acoustic meatus. as well as bring fibers secretarial For glandular sub maxillary and sub lingual. After go out from bone mastoid, nerve facialist going to parotid gland and divides to innervate the facial muscles. 8,9
3. Fracture Bone Temporal
Epidemiology
Motor vehicle accidents result in head trauma of various types. level severity. In time Then, 75% from accident vehicle motorized resulting in trauma head, However moment This Already reduce with seat belt usage and the emergence of airbags . Although the force of trauma is not strong enough to break the skull, 14%-22% of sufferers experience temporal bone fractures. It has been reported that up to now 31% of fractures are caused by motor vehicle accidents. Facial nerve paralysis occurs in 20% of sufferers, usually in the form of neuropraxia or partial axonotmesis . Temporal bone fractures have been reported to occur in all age groups. More than 70% occur during the second, third and fourth decades. Fractures mainly occur in men with a ratio of 3:1, due to involvement in risky activities rather than due to structural weaknesses in the male skull. 6,8,10
According to Bailey 11 , about 6-7% of cases of temporal bone fractures in adults will be accompanied by facial nerve injury. While in children the incidence is around 3-9%. From Hough, 75% of head trauma patients with middle ear damage are men, while women are 25%. 10
Type Fracture Bone Temporal
Temporal bone fractures consist of longitudinal fractures, transverse fractures and fracture mixture or combination. Clash from direction frontal And occipital often causes fracture transversal And clash from lateral cause fracture Longitudinal. Longitudinal fractures are the most common, usually from the mastoid segment across the roof of the Eustachian tube or starting from the foramen magnum and running towards the ear canal. The fracture line is parallel to the axis of the petrous pyramid and usually runs along the anterior wall of the pyramidal pars, so that the labyrinth and facial nerve are often spared from the lesion. These fractures are usually linear, If branching can to be continued to hole ear or mastoid, seldom to inner ear. In other words, this fracture is usually a middle ear fracture. The tensor tympani muscle can be severed, so that incus dislocation is often found. Around 30% sufferer with fracture longitudinal there is disturbance deaf conduction.2.10- 15
The transverse fracture starts from the jugular fossa across the pyramid to its anterior surface and causes hemorrhage in the cochlea and semicircular canals. The middle ear remains intact, unless the fracture is extensive through its medial wall. Small fractures Which extend into mastoid or antrum can result in ecchymosis around the mastoid. The facial and vestibulocochlear nerves can be damaged by laceration or compression. Transverse fractures can cause sensorineural hearing loss, vertigo and account for 50% of cases of paralysis. facial nerve. Fracture location facial nerve labyrinth segment approximately 90% and the meatal segment 10% of cases. 10,15,16

Picture 4. Fracture longitudinal bone temporal (left) And fracture transverse temporal bone (right)
4. Neurophysiology And neuropathology injury nerve
Facial expression is the result of 7000 motor fibers moving in sync which initiates muscle contractions. Each axon synapses with several fibers. Chemical neurotransmitters such as acetylcholine and enzymes of the choline transferase group are formed by the nerve body in the pons and transported along the nerve going to laminate end motor or motorbike end plate, through microtubular system. The facial nerve has a single motor neuron located in the central nervous system. The axon of the motor cell is wrapped by Schwann cells and forms a neural tubule. The nodes of Ranvier which are the boundaries between Schwann cells can be seen every one millimeter. The axon receives oxygen from the Schwann cells And help its axoplasm from neuron parent. Speed The metabolism of axoplasm and its movement speed is estimated to be around 1 mm per day. Its development starts from the central nervous system towards the distal, this is the speed of regeneration of an axon when a nerve is completely cut. 7,8,9,13
Seddom classifies facial nerve paralysis into 3, namely neuropraxia, axonotmesis and neurotmesis. While Sunderland divides facial nerve paralysis into 5 different classes. Class I injury is called neuropraxia, where there is a conduction block due to the cessation of axoplasmic flow Because compression. It is expected happen recovery full on injury this. Class II is called axonotmesis, the axon is disrupted and Wallerian degeneration occurs distal to the injury site. The endoneural tube remains intact, so regeneration can occur, but is very slow at 1 mm per day. There is still a possibility of complete recovery of function in class II injuries. Class III injuries are called neurotmesis. In injury This tube nerve disturbed so that regeneration back and function is affected. If regeneration does not occur, synkinesis is likely present. Synkinesis is the abnormal movement of muscle masses together. Injuries class IV classified as disturbance endoneurium, perineurium and axons, whereas epineurium still intact. Results regeneration poor functionality, with a high risk of synkinesis. Grade V injuries are the worst and are classified as complete nerve damage. There is little chance of regeneration. The risk of neuroma formation is increased due to axonal sprouts that make their way go out from the sheath nerves. 5,6,7,8
Table 1. Neuropathology And Healing Spontaneous Which Related with Facial Nerve Damage Grade 5
Overview of the Degree of Damage Nerve | Pathology | Neuron Healing | Healing Time | Spontaneous Healing After 1 year |
Degree I
| compression . None. change morphology. (neurapraxia) | No morphological changes | 1 – 4 weeks | According to House- Brackmann (HB) I: completely recovered without wrong regeneration. |
Grade II
| Persistent pressure. Increased intraneural pressure. Axons missing but endoneurium intact (axonotmosis) | Axons travel along the intact endoneurium at a rate of 1 mm/day. | 1 – 2 months | HB II: moderate healing (visible difference in movement) consciously or spontaneously). |
Grade III
| Intraneural pressure increases, endoneurium is damaged (neurotmesis) | Axon may grow off course because the endoneurium is open so that it can occur synkinesis. | 2 – 4 months | HB III – IV: healing is poor ( imperfect healing or deformity, synkinesis is evident) currently heavy) |
Grade IV
| Like III degree But accompanied by damage to the perineurium (partial rupture) | The regeneration process is hampered by the presence of connective tissue. | 4 – 18 months | HB V: obvious weakness face. Synkinesis, spasm rarely or There isn't any. |
Degree V
| Like degree III & IV accompanied by rupture of the epineurium (total rupture) | There isgaps filled with connective tissue inhibit axon growth and innervation muscle. | No Happen | In accordance HB VI: no healing (tone lost) |

When the impulse is blocked, neuropraxia or conduction block occurs, there is a blockage of the flow of axoplasmic transport in both directions, but some axoplasmic transport continues. The distance between the injury site and the cell body in punch follow determine level injury to overall nerve. If injury occurs in the internal acoustic canal with axons severed, then the lost axoplasm will be quite long and permanent damage will be greater compared to damage that occurs distally, near the motor end plate.
Person Which more young will healed more perfect from injury Which the same when compared to older people. If the magnitude of pressure on the nerve is sufficient to cause complete obstruction of axoplasmic movement through the injury site for several days, then axonotmesis occurs with loss of axonal continuity. As a result, Walleri's degeneration occurs in the distal part.
During a number of day axon Still can responsive in a way electric to external stimuli in the distal part, but not There is voluntary motor movement or electrical conduction through the injury site. Histologically the proximal nerves are still normal but biochemical changes have occurred. 8,9
Schwann cells swell and are phagocytic, then divide until they completely fill the tubule. connecting network that surrounding each nerve fiber. Neurons that are deprived of nutrients will return to their original size after the axon loses Nissl substance by cytoplasmic swelling or chromatolysis. Three or four days after injury occurs formation tape Bunker. Tape This allegedly provide substance biochemistry for the nerves Which new. When fiber nerve cut off, nerve Which experience repair forms a growth cone at the proximal end of the axon. There are multiple protoplasmic processes in the growth cone and the single regenerating axon grows branching and enters the Schwann cells of various tubules. In the same way growth can occur towards other nerves. 6,8,9
Facial muscles can undergo wasting away after the loss of motor nerves. facialist pass three stages injury. Stage First in progress until 21 days, involving physiological events where the cell body undergoes metabolic transformation. And start regenerate use to form axoplasm Which will occupying the neurotubules. The second stage lasts up to 2 years, a period during which cells and proximal segments can regenerate using Brugner's bands or endoneurial tube reserves, through which regenerated axons can reach the facial muscles. Therefore, up to 2 years after injury, reanastomosis of the severed nerve can still be considered by placing a connecting graft between the 2 separated points or transferring a functional motor nerve to the distal nerve segment. For this reason, it is believed that facial muscle rehabilitation can be done by nerve transfer or reanastomosis. injury nerve, at least in term time 24 month after injury. The third stage is usually characterized by scarring of the distal nerves and muscle degeneration. 7,8
Histochemical analysis of regenerating neurons showed increased levels of RNA synthesis and glucose-6-phosphate dehydrogenase that peaked at about 21 days. Some experts say based on the information This, that nerve Which cut off will healed most Good when repaired as soon as possible. Delay is not recommended because it can cause physical changes and scar tissue formation in the wound. 8,9,17
5. Determining the Height of Facial N Lesions (N.VII)
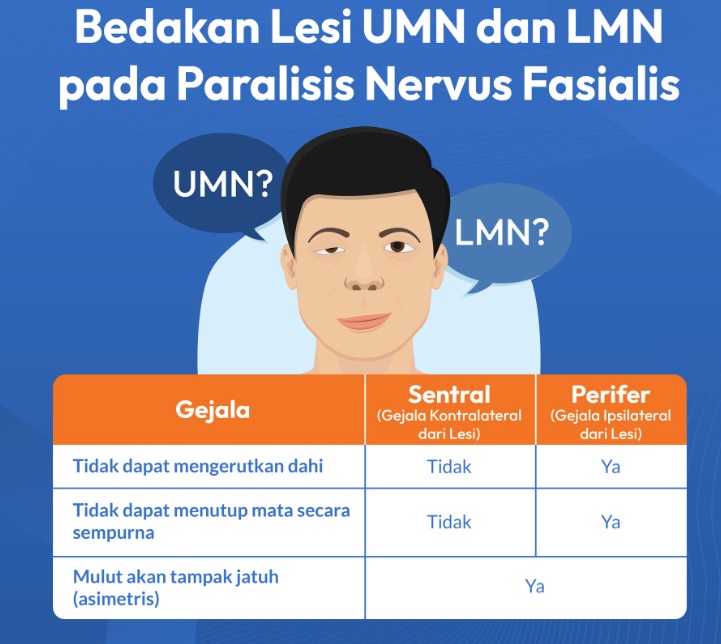
A. Determining Upper Motor Neuron or Lower Motor Neuron Lesions by means of
B. If the Lower Motor Neuron determines how high the lesion of the facial nerve is by:
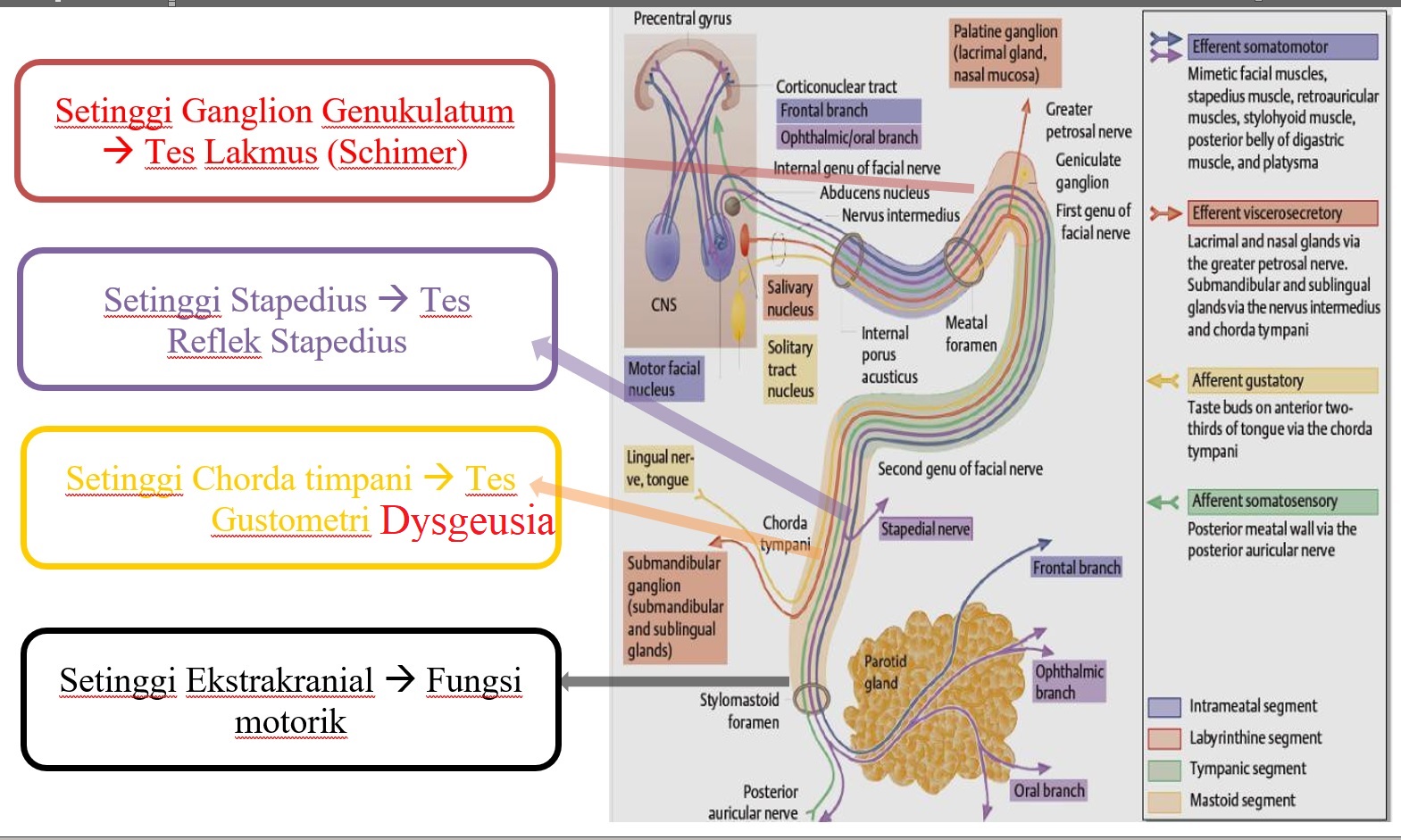
The Schirmer test is a test used to check if the eye is producing enough tears to keep it moist. This test is used when a patient is experiencing dry eyes or excessive tear production. This test is not invasive or damaging to body tissue. A normal result for this test is negative with more than 10 mm of wet filter paper for 5 minutes. Both eyes should produce the same amount of tears.
reflex test or acoustic reflex test is a non-invasive audiology procedure that evaluates the ear's response to loud sounds. This test is performed to assess the health of the auditory system, including the outer, middle, and inner ears, and the areas of the brain that connect them.
Gustometric Test Taste is the main sensory system that keeps a check on ingested food. Human beings are able to recognize five basic tastes: salty, sour, sweet, bitter and umami. Gustometry, including both gustometry with application of taste substances and electrogustometry, is the method of taste examination. There are various methods of applying taste substances during gustometry examination. The stimuli used in gustometry are: citric acid or hydrochloric acid (sour taste), caffeine or quinine hydrochloride (bitter taste), sodium chloride (salty taste), saccharose (sweet taste), monosodium glutamate (umami taste). Electrogustometry, widely used by clinicians to examine taste sensitivity, allows to estimate the functioning of taste by means of electric excitability thresholds determined through the response to the irritation of taste buds area with electrical current of different intensity. Electrogustometry is especially useful in estimating the efficiency of sensory pathways. However, if we want to examine taste sensitivity to individual taste categories we should use more laborious gustometry with the application of taste substances, whose main advantage is the use of physiological stimuli.
Dysgeusia
Dysgeusia due to injury to the chorda tympani nerve can be quite distressing for some patients. Symptoms such as a metallic taste in the mouth usually improve with time, but patients should be warned that these taste changes may persist. This is of particular concern for patients who require a keen sense of taste in their profession. Trauma to the chorda tympani nerve tends to result in long-lasting dysgeusia.
6. Diagnosis
Head injuries caused by motorcycle accidents are the most common cause case paresis nerve facialist consequence trauma (31%). Mechanism or detailed history from trauma must asked on anamnesis. Including part head affected collision. This relate with the possibility type fracture Which happened. Trauma from direction frontal or occipital often cause fracture bone temporal transverse type. While trauma from the lateral direction often causes longitudinal fractures. The onset and progression of facial nerve paresis are very important. The presence of hearing loss or vertigo after temporal bone trauma should be suspected of having injured the facial nerve. As soon as the patient's general condition and hemodynamic function are stable, an examination of the facial nerve and hearing status is performed. Including an initial examination with otoscopy. Often the initial examination For function nerve facialist This late Because “condition emergency” like
active bleeding is considered to have resolved. ENT examination of the ear includes examination of the external acoustic canal, looking for lacerations or injuries. With the help of an otoscope, see the condition of the tympanic membrane, whether it is accompanied by perforation or hemotympany. Take note Also type fluid autore Which out, whether it is mixed with blood or clear (cerebrospinal fluid). 6,7,8
Table 2. Degrees paralysis nerve facialist based on House and Brackmann 7
Degrees | Description | Characteristics |
I | Normal | Function facial normalon all area |
II | Mild Dysfunction | Mild weakness is seen on inspection of near Possible there is Mild synkinesis Symmetrical And tone Restnormal Movement : Forehead: medium function until good Eye: closeperfect with Minimum effort Mouth: light asymmetric |
III | Moderate Dysfunction | Clear but not visible difference in shape means; seen But No there is synkinesis, contracture or spasm hemifacial Whichheavy Symmetrical And tone Restnormal Movement: Forehead: mild to moderate Eyes: close with business Mouth: weak withmaximum effort |
IV | Moderate-Severe Dysfunction | Weakness clearor asymmetric clear Symmetrical and normal resting tone Movement : Forehead: There isn't any Eye: closeNo perfect Mouth: asymmetric withmaximum effort |
V | Severe Dysfunction | Only A little movement Which looks Asymmetrical at rest Movement : Forehead: There isn't any Eye: close No perfect Mouth: little movement |
VI | Paralysis Total | No There is movement The same very |
Complications other from damage nerve facialist is water eye crocodile tears ), Which happen consequence deviation regeneration fiber nerve parasympathetic Which should innervate gland saliva, become deviate to the lacrimal gland. In addition, hyperkinesis can also occur in the stapes tendon, which causes complaints of fullness and rumbling in the ears. The purpose of examining the function of the facial nerve is not only to determine the degree of paralysis, but also to determine the location of the facial nerve lesion. In examining the motor function of the facial muscles, the gradation of facial nerve function according to House-Brackmann and Freys can be used.7,8
In the Freys grading system, which was first introduced in France, there is a slight difference with House Brackmann. In this system, 4 components are assessed, namely motor function examination, tone, synkinesis and hemispasm. In the motor system examination, the face is divided into 10 areas, based on 10 muscles responsible for facial expressions and facial expressions. The ten muscles examined and how to examine them are explained in table 2.7,8
Table 3. Method inspection muscle face
Muscle | Method inspection |
|
|
In condition normal, Where No there is abnormality nerve facialist, then the value maximum from summation 10 area in face on One side is 30. Inspection facial tone is assessed by dividing the face into 5 areas. According to Freyss, tone testing is important and assessment does not have to be done for every muscle, but rather for each level of facial muscles. Mark For tone worth 0-3, with mark 3 For tone normal And 0 when there is no tone. If there is hypotonus, the value is reduced by 2 for each level depending on the degree. Under normal circumstances the total value for the tonus of the five levels face is 15. Synkinesis is Wrong One complications from facial nerve paresis. To find out whether or not there is synkinesis, the following examination is carried out: a) The patient is asked to close his eyes as strong as possible, Then examiner notice There is whether or not movement muscles in the area corner lips on. Then done evaluation as following: mark 2 if no synkinesis is found. If synkinesis occurs on the paretic side, depending on the degree, the value is reduced by 1 or 2. b) The patient is asked to laugh out loud while showing their teeth, then the examiner observes whether or not there is movement of the muscles in the lower eye corner. Assessments such as (a). c). Synkinesis can also be seen moment somebody speak (movement emotion). Examiner pay attention to the presence or absence of muscle movement around the mouth. If there is no synkinesis, a score of 1 is given. If there is synkinesis on the paretic side, a score of 0 is given. Hemispasm is a unilateral facial nerve hyperactivity. If there is no hemispasm, a score of 0 is given, but if there is hemispasm, a minus one (-1) value is given for each movement. The total value of motor, tone, synkinesis And hemispasm on condition normal is 50. Gradation paresis, assessed based on the total value of the examination results multiplied by 2 to obtain the percentage of facial nerve motor function. good. In this system, topographic assessment and electrophysiological test examination are also carried out, including the Nerve Exitability Test (NET), Maximal Stimulation Test (MST), Electroneurography (EnoG) and Electromyography (EMG). Topographic assessment includes the Schirmer test, stapedius reflex and gustometry. The Schirmer test or nasolacrimal reflex test, to determine function fiber sympathetic nerve facialist through nerve petrosus superficial at the level of the geniculate ganglion. The method is to place litmus paper on the base of the conjunctiva. According to Freys, if there is a difference between the right eye and left, ≥ 50% considered pathological. For evaluate reflex stapedius used electro caustic impedance is by providing a threshold of stimulation on m.Stapedius to determine the function of the stapedius nerve, a branch of the facial nerve. In gustometry, the difference in the threshold of stimulation between the right and left is assessed. Freys determined that a difference of 50% between the two sides is pathological. From this system, the location of the lesion can be reported with the best percentage of motor function along with the possibility of prognosis from the results of NET, MST, EnoG or EMG. 7,8,9
The examination of nerve weakness can also be checked with the Portman Index. This index observes the branches of the facial nerve that innervate the facial muscles. in hair temporalis, zygomatic, buccal, mandibular And cervical. The severity is assessed based on the motor function and tone of the muscles so that it will determine the reversibility of the paralysis. The assessment is done by frowning, closing the eyes, lifting and wrinkling the nose, whistling, laughing out loud and grimacing. The assessment of each nerve branch is assessed using the Portman index. If the patient cannot be assessed 0, a little can be rated 1, more Can rated 2 And normal rated 3. On examination tone, normal tone is assessed as 2, then added up and the result is divided by 20 and multiplied by 100%. If the result is >60% then the prognosis is good. 18
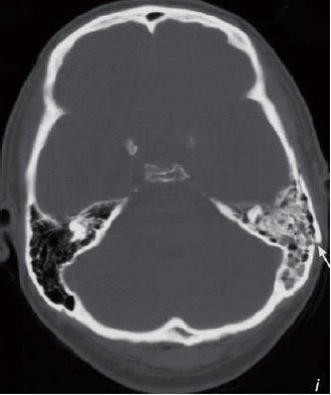 Radiological examination in the form of high-resolution CT scanning is very helpful in confirming the diagnosis of bone fractures. temporal. The integrity of the ossicles or auditory bones is also evaluated. If possible, to obtain maximum imagery, the CT scan requested is a coronal axial section with a slice of 0.6 mm.
Radiological examination in the form of high-resolution CT scanning is very helpful in confirming the diagnosis of bone fractures. temporal. The integrity of the ossicles or auditory bones is also evaluated. If possible, to obtain maximum imagery, the CT scan requested is a coronal axial section with a slice of 0.6 mm.

Picture 5. CT Scan piece Axial, looks fracture bone temporal left
Hearing tests are performed if the patient's condition allows, starting from simple audiological examinations in the form of tuning tests, pure tone audiometry and tympanometry. In addition to functioning to detect the degree of deafness that occurs, this examination is important as a basis for the development of treatment progress after surgical therapy is performed. Electrophysiological tests such as NET, MST, EnoG and EMG are performed to assess the degree of damage, determine the prognosis for facial nerve repair after trauma and plan the therapy to be given. 7,8,9
7. Management
Management paresis nerve facialist consequence fracture bone temporal Until now it is still a controversial issue. Schematically, the treatment of facial nerve paralysis due to temporal bone fracture is explained in table 4: 7
Conservative
Conservative treatment given is medication and physiotherapy. Treatment to reduce nerve edema can be given corticosteroids. Neurotonics are given for nerve growth. Physiotherapy also can given covering infra red radiation (IRR), electrical stimulation (ES), deep kneeling exercise and mirror exercise . All of the above efforts aim to maintain muscle contractility. The masses reported that patients with facial nerve paralysis without any poor prognostic factors would experience complete improvement and healing. In patients with facial nerve paralysis nerve level I And II House And Brackman obtained more from 90% of patients experienced improvement approaching normal. 6,8,19,20
Surgery
Some authors recommend observation and symptomatic therapy only. Mainan et al., observed 45 non-operative patients, found that 44 people experienced satisfactory healing and 65% experienced healing that perfect. Like quoted Mattox, from McKennan and Chole, patients with late-onset facial nerve paralysis, continued to experience healing Which Good. When has decided patient with paresis. The facial nerve due to trauma will undergo surgical therapy in the form of decompression, the patient is faced with a situation between rapid onset or slow onset. has long. On onset Which fast, usually condition trauma patient more severe. From Mattox, different from what was obtained by Adegbite et al., said that the prognosis is more determined by the degree of facial nerve damage, not by time or onset. According to Fisch, based on the results of electrophysiological tests (EnoG), degeneration of nerve cells began to occur 6 days after onset.
Table 4. Chart Handling paralysis nerve facialist

Ideally, decompression is performed immediately after the trauma occurs. But according to Fisch and Kartush, the best time to perform this decompression surgery is after 3 weeks, because edema and tissue hematoma have been minimal, intraoperative bleeding is minimal so that the surgical field is more clearly visible. Although repair within 30 days after trauma shows the same results. In cases of facial nerve paresis that have lasted a long time, electrical or physiological tests no longer produce valid results. It is recommended to wait up to 12 months, after which surgery is performed if there is no clinical improvement or the EMG results are also not good. Surgical exploration facial nerve post trauma need surgeon who is experienced in mastoid surgery, translabyrinthine, middle fossa exploration and nerve repair. Accuracy during surgery is very necessary, because according to Jones, 14 out of 15 patients with CT scanning bone fracture temporal, also accompanied by ipsilateral temporal lobe contusion. The success of nerve surgery is greatly influenced by knowledge of facial nerve anatomy, the availability of intraoperative electrical monitoring devices and the completeness of the instruments.
Surgery is performed if there is severe hearing loss and disturbances. balance. Procedure operation is to free nerve, nerve decompression or repair in a way anatomy nerve facialist. According to Hough that 66.6% of patients trauma head new found existence line fracture moment operation ongoing, 92.3% happen dislocation incudostapedial as well as 57.1% bone incus has let go from its place. Surgical action can be performed with 3 approaches depending on the type of trauma and the location of the affected facial nerve. The approaches that can be performed are: 1) mastoidectomy or extended mastoidectomy approach, 2) medial cranial fossa approach and 3) transmastoid approach. 7,15-22
Approach mastoidectomy or extended mastoidectomy done to observe the facial nerve from the geniculate ganglion to the stylomastoid foramen that is on segment timpani And segment mastoid. Approach This can clearly identify the Fallopian canal. The surgical procedure is first a simple mastoidectomy is performed, second a recess is traced and identified. facialist, third identification segments nerve And network canal facialist, fourth remove bone wrapping nerve And fifth If indicated to perform nerve sheath opening.
To observe the facial nerve section from the distal geniculate ganglion properly, a wide mastoidectomy can be performed. The medial cranial fossa approach is performed to observe the entire labyrinthine segment of the facial nerve from the geniculate ganglion to the internal auditory canal. This procedure is used not only for facial nerve exploration, but also for small intracanalicular acoustic neuromas and to explore the vestibular nerve. Procedure action This combined with approach trans mastoid then done exploration on area process cochleariform with petrous nerve superficial major as landmarks . Difficulty approach This is
1) existence leakage dura mater with herniation And damage bone temporal, 2) avulsion nerve petrosus superficial major, 3) bleeding artery meningitis medial, and 4) cochlear trauma or superior semicircular canal trauma.
This transmastoid approach can expose 60% of the labyrinthine segment. In addition, according to May, the rate of facial nerve paresis improvement is also higher, namely 84-85%. The transmastoid approach itself has 2 methods, namely 1) transmastoid epitympany where the incus is removed during surgery and then reinstalled. 2) transmastoid epitympany and otoendoscopy where the incus is only shifted up or down.
Following is step – step decompression nerve facialist transmastoid 23.24
Drill the mastoid cortex with the landmarks of Mc Ewen's triangle, identifying the posterior wall of the ear canal, the temporal line and the spine of Henle. Clean and remove all air cells from the antrum. to the mastoid tip and digastric ridge found. Identification tag mastoid, sine sigmoid, semicircular canals lateral, adit ads antrum, fossa incudis, solid angle. Aircell in the area The zygoma root is also removed until identified. upper edge of the incus and the horizontal part of the facial canal. Landmarks for N. Facialis pars vertical is the posterior tip of the incus at the top and the anterior end of the digastric groove at the bottom. lower. Drill until foramen stylomastoid. Bone between foramen stylomastoid And canal semicircular lateral thinned out And until N.facialis appears pink. If there is pathological tissue/granulation tissue, it is cleaned.
If the horizontal segment of N.VI is affected, decompression is performed through the triangle (posterior tympanotomy) formed by the medial N.VII. , cord timpani And annulus timpani in lateral and short process incus in superior part. Identify the incus, incudimalleolar joint and malleus and check the mobility of the ossicles and patency of the aditus ad antrum. If the entire horizontal segment must be decompressed, the incus must also be disarticulated.
Open Channel facialist And sheath nerves
Landmarks of the external genu, chorda tympani and facial recess are visible. Thinning of the facial canal is done using a diamond drill so as not to injure the facial nerve. From the external genu to the stylomastoid foramen.
After the facial nerve pars tympani and pars mastoid are exposed, identify the damage to the nerve according to the topography of the lesion. Thin the bone on canal facialist until bone thin the can lifted using a micro elevator.
Done appointment bone thin along nerve facialist on 3 aspect : 1) descending portion of the mastoid segment between the stylomastoid foramen and the external genu on the posterior aspect, 2) the external genu and facial recess portion on the lateral aspect and 3) the horizontal segment to the inferior edge of the cochleariform process .
With the facial nerve landmark, open the sheath of the nerve, carefully. sharp sheath incision with technique atraumatic and preservation of the entire nerve fascicle. Ziegler ophthalmic knife can be used for nerve sheath incision.
Identification nerve facialist : clean up hematoma, flakes bone or nerve damage to the lesion topic. So that there is no pressure on the facial nerve. Cover with fascia graft.
Placed tampon hole ear Which Already coated by ointment antibiotics.
Wound operation closed with stitches layer layer by layer
When need installed pipe Salir in the area incision
Decompression procedures can be used to repair damaged nerve tissue. disconnected with method connect back to continuous axon nerve. If the nerve damage is not extensive, the edges of the nerve can be sharply divided and then repositioned. anatomically nerve. If the edge nerve No can taken or if the nerve part No can renovated so graph nerve can installed. If nerve facialist Severe damage can be treated by grafting or cable grafting or by complete end-to-end anastomosis . Nerve grafts can be taken from the matrix. or part axon nerve Which installed from proximal until the part distal nerve. Grafts that are often used are from the branches of the superficial cervical plexus, especially the greater auricular nerve, because the grafts are easily obtained around the surgical site and the size is suitable. 5,7,16-22
Procedure taking auricle graft major is as following: perpendicular line marker to the line between the mastoid tip and the angle of the mandible. It is located just below the platysma muscle, above the sternocleidomastoid muscle. Then an incision is made on the skin that has been marked, followed by careful release of the graft. The graft is cut after the facial nerve preparation is complete .
Another location for nerve grafting is the sural nerve graft. The procedure is almost the same as the auricle graft, but what needs to be considered is the location of the graft and patient preparation. Nerve identification is estimated 2 cm behind And 1-2 cm proximal from lateral malleolus. The dissection of the medial sural nerve is proximal below the popliteal fossa. There is a nerve of 30-35 cm for grafting. Next, the nerve is transected proximally and wrapped with a moist gauze swab . 23.24
The most important aspect of nerve repair is ensuring that the endoneurial segments are aligned as this will promote regeneration. The nerve ends should be sutured using 9-0 or 10-0 monofilament suture to connect the epineurium or perineurium. Complications of action operation can happen bleeding. Bleeding the can overcome with cautery and covered with bone wax .
According to Salinas JD, that giving injection corticosteroids on joints and soft tissue due to trauma will accelerate healing. Corticosteroids work by limiting capillary dilation and permeability of vascular structures, so that the inflammatory process can be inhibited. Corticosteroids also inhibit the formation of arachidonic acid as a material for making prostaglandins. As a result of the action decompression nerve happen lost hearing type conduction more from
15 dB which occurs in 14% of cases. Conductive hearing loss is caused by by fixation stapes Because fraction bone, herniation dura mater affecting the top of the malleus head or due to disarticulation of the incudomaleus joint.
8. Prognosis
The prognosis of facial nerve paralysis due to temporal bone fracture depends on the type of fracture, clinical symptoms that arise, the time of trauma and its management. Factors that cause a poor prognosis are acute symptoms or paralysis occurring immediately after trauma, complete paralysis in the form of neurotmesis where the nerve is severed during trauma. In facial nerve paralysis, if there is improvement in the first 3 weeks, the prognosis is expected to be good.8
According to May and Shambaugh, in grade 1 trauma, facial nerve repair begins to occur within 1-4 weeks and spontaneous healing is possible. 1 year after trauma. Trauma degrees 2 will healed with satisfying or happen symptom remainder minimum, start happen repair in 1-2 month. Degrees 3 no experience healing that perfect, start happen repair in 2-4 months. Degrees 4 happen process repair start 4-18 month And degrees 5 No healing occurs. Most deaths in temporal fractures are caused by increased pressure intra cranial in a way I. Three principle treatment paresis Acute facial nerve is physical therapy, drug therapy and psychophysical therapy. Patients are still advised to check at 1 week, 3 months, 6 months and 1 year after surgery to examine the function of the facial nerve. 5,6,8,9,25
REFERENCE
Amen Z, Sayuti R, Kahairi A, Reconciliation W, Ahmad R. Head Injury with Temporal Bone Fracture: One Year Reviews of Case Incident, Causes, Clinical Features and Outcomes. Med J Malaysia. 2008:373-6.
Liston SL. Duvall AJ. Embryology, anatomy and physiology of the ear. In: Adams GL, Boies LR, Hilger PA, editor. Book Teach Disease ENT. Edition 6. Jakarta: EGC; 1997: 27- 38.
Gordin E, Lee TS, Ducic Y, Amaoutakis D. Facial nerve trauma: evaluation and considerations in management. Craniomaxillofac Trauma Reconstruction. 2015;8:1–13.
Gleinser D, Makishima T, Quinn FB, Quinn MS. Facial Nerve Trauma. UTMB Dept. of Otolaryngology. 2009:1-11.
May M, Schaitkin BM, Barry M et al. Trauma to the Facial Nerve: External, Surgical and Iatrogenic. In: May M, Schaitkin BM, editors. The Facial Nerve. Edition 2. New York: Thieme; 2000: 367-82.
Vrabec JT, Coker NJ. Acute Paralysis of the Facial Nerve. In: Bailey BJ, Johnson JT et al, editors. Otolaryngology Head and Neck Surgery. 2013.Philadelphia : Lippincott Williams & Wilkins; 2014: 2139- 54.
Soefferman R. Facial nerve injury and decompression. In: Nadol J, Mc Kenna M, editor. Surgery of ear and temporal bones. Edition 2. Philadelphia: Lippincott Williams & Wilkins; 2005: 435-50.
Austin D. Facial nerve paralysis. In: Snow JB, Ballenger JJ, editors. Ballenger's otorhinolaryngology head and neck surgery. 17th ed. New York: McGraw Company; 2009: 554-65.
Maisel RH, Levin SC. Disturbance nerve facialist. In: Adam GL, Boies LR, Higler PA, editor. Book teach disease ENT. Edition 6. Jakarta : EGC; 1997: 139-152.
Hough JVD, McGee M. Otologic Trauma. In: Paparella MM, Shumrick DA et al, editors. Otolaryngology Head and Neck Surgery. 6th ed. Philadelphia: WB Saunders; 1991: 1137-60.
Diaz R, Brodie HA. Middle Ear and Temporal Bone Trauma . In: Bailey BJ, Johnson JT et al editors. Otolaryngology Head and Neck Surgery, 4th Ed Vol 1. Philadelphia : Lippincott Williams & Wilkins, 2006. p. 2057-79.
Coker NJ, Vrabec JT. Acute paralysis of the facial nerve. In: Bailey BJ, editor. Head and Neck Surgery-Otolaryngology. Edition 5. Philadelphia: Lippincott Williams & Wilkins; 2014: 2139-54.
Kerr AG. Smyth G. Ear trauma. In: Booth J, editor. Scott's Browns Otholaryngology Otology. Edition 5. London: Butterworth & Co;.1987: 172-84.
Hat N, Note J, Hakuba N, Gyo K, Yanagihara N. Facial nerves decompression surgery in patients with temporal bone trauma: analysis of 66 cases. J Trauma. 2011;71:1789-92.
Kumar A, Bar A, Patni A. Evaluation of facial paralysis. In: Nadol J, Mc Kenna M, editors. Surgery of the ear and temporal bone. Edition 2.. Philadelphia: Lippincott Williams & Wilkins; 2005: 69-77.
Coin AM, Hurvitz KA, Evans RD, Wirth GA.Facial paralysis for the plastic surgeon. Can J Plast Surg. 2007;15:77-82.
Gleinser D, Makishima T, Quinn FB, Quinn MS. Facial nerve trauma. The University of Texas Medical Branch J. 2009;1-11.
Widuri A. Facial Nerve Paresis in Chronic Suppurative Otitis Media Unsafe Type. Vol. 5. 2010. P. 132-8
Brodie HA. Management of Temporal Bone Trauma. In: Flint PW, Haughey BH, Lund VJ, Niparko JK, Richardson MA, Robbins KT, Thomas K, Thomas JR, editor. Cummings Otolaryngology Head & Neck Surgery. 5th Edition. Philadelphia: Mosby Elsevier; 2010: 2840-71.
Hat N, Note J, Hakuba N, Gyo K, Yanagihara N. Facial nerves decompression surgery in patients with temporal bone trauma: analysis of 66 cases. J Trauma. 2011;71:1789-92.
Cameraman DB, Thompson SW. Middle Ear and Temporal Bone Trauma. In: Bailey BJ, editor. Head and Neck Surgery-Otolaryngology. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2014: 1773-85.
Said BM, Hughes GB. Surgery for traumatic middle ear condition. In:Habermann RS, editor. Middle Ear and Mastoid Surgery. New York: Stuttgart Thieme; 2004: 143-150.
Anderson RG. Facial Nerve Disorders and Surgery In Selected Readings in Plastic Surgery. Vol 10 number 14, 2006. University of Texas Southwestern Medical Center at Dallas.
Sainsbury D, Borschel G, Zuker R. Surgical Reanimation Techniques for Facial Palsy/Paralysis. In Open access atlas of otolaryngology, Head and Neck Operative Surgery, 2005. www.entdev.uct.ac.za.
Patel A, Groppo E. Management of temporal bone trauma. Craniomaxillofac Trauma Reconstruction. 2010;3:105–13.
Sanus GZ, Tannover N, Tanriverdi T, Uzan M, Root Z. Late decompression in patients with acute facial nerve paralysis after temporal bone fracture. Turk Neurosurg. 2007;17:7-12.
Massa N, Westerberg BD. Facial Nerve, Intratemporal Bone Trauma. Available from URL: http://emedicine.medscape.com/article/846226- overview, Article Last Update Jan 26, 2009. April 2009.
Schwaber MK. Trauma to the Middle Ear, Inner Ear, and Temporal Bone. In: Ballenger JJ, Snow JB, editors. Otorhinolaryngology Head and Neck Surgery, 16th Ed. Baltimore: Williams & Wilkins, 2003. p. 345-56.
Salinas JD, Rosenberg JN. Corticosteroid Injections of Joints and Soft Tissues. Available from: URL http://emedicine.medscape.com/article/325370- overview. Article last updated January 15, 2020
Comments