APPROACH MANDIBULOTOMY AND RECONSTRUCTION WITH PECTORALIS MAJOR MYOCUTANEOUS FLAP IN SQUAMOUS CELL CARCINOMA OF THE TONGUE
I Made Nudi Arthana
On SCC (Squamous Cell Carcinoma) cavity mouth ( tongue ), distribution type gender varies according to age of onset: while males account for more than 70% of cases on person old, the percentage down become 50-65% in lower age 45 years. Intervention surgery in treatment cancer mouth can use mandibolotomy with pectoralis flap.
LITERATUR REVIEW
Anatomy Tongue
Tongue own four function main: (1) digestion mechanical through compression, abrasion, And distortion, (2) manipulation For help chew and preparing food for swallowing, (3) sensory analysis with touch, temperature, and taste receptors, and (4) secretion of mucin and lingual lipase enzymes. The tongue is divided become part front And root posterior. Back tongue contain numerous fine projections known as lingual papillae. Each papilla has an epithelial lining squamous layered thick, Which give friction addition which helps the tongue in moving the materials around it. In addition, Tastebuds there is in throughout edge Lots papilla. Line shaped V rough from circular papilla show limit between body And root tongue, Which located in pharynx. 7.8 Epithelium tongue wetted by water, season, And lipase lingual, Which is a secretion from small glands that extend into the lamina propria. Lingual lipase initiates the enzymatic breakdown of lipids, especially triglycerides. The epithelium lining the inferior surface tongue more thin And more fine than back. In throughout line inferior middle is the frenulum of the tongue, a thin fold of mucous membrane that connects the body tongue to mucosa floor mouth. Channel from two pairs of salivary glands open on each side of the frenulum, which regulate extreme tongue movement. However, frenulum Which too strict can hinder Eat or speak. Condition This, Which known as ankyloglossia, can corrected through
procedure surgery. 7,8

Picture 1. Anatomy Tongue. 8
Gustation, known as the sense of taste, provides information about the food and drinks we consume. Taste epithelial cells, or taste receptors, found in the taste Which spread in on surface tongue, and the adjacent parts of the pharynx and larynx. These cells are activated by food molecules, which trigger action potentials that are sent to the taste cortex for interpretation. The surface of the tongue has numerous epithelial projections called lingual papillae. These papillae function as mounds small Which shaped nipples. There is four type papilla lingual, that is filiform papillae (from the Latin word "filum" meaning thread), fungiform papillae (from the Latin word "fungus" meaning mushroom), vallate papillae (or sometimes called lentiform papillae), and foliate papillae (from the Latin word "folium" meaning leaf). There are regional differences in the distribution of papillae on the tongue. 8

Picture 2. Gustasi And Papilla Tongue. 8
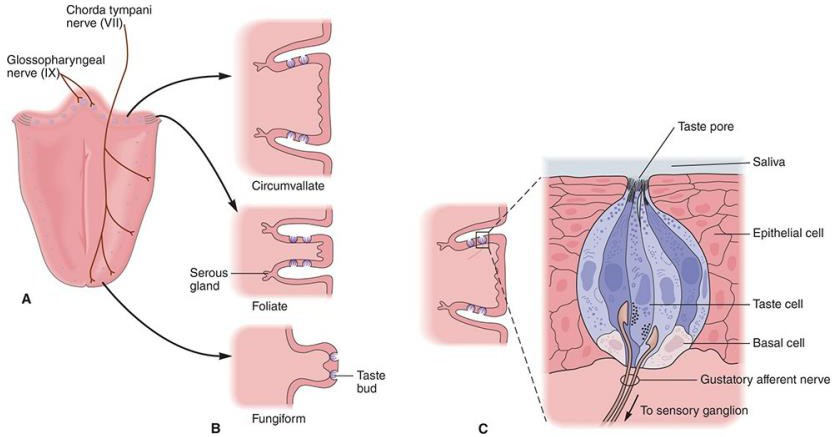
Figure 3. Tastebuds are located on the papillae of the human tongue. A) Taste. Tastebuds in the anterior two-thirds of the tongue are innervated by the chorda tympani branch of the facial nerve; whereas Which located in one third part behind tongue innervated by lingual branch of the glossopharyngeal nerve. B) Three main types of papillae ( circumvallate, foliate, and fungiform ) are found on different parts of the tongue. C) Tastebuds consist of basal stem cells and three types of taste cells (dark, light, and transition). Cells taster This elongated from base Tastebuds to taste pores, where microvilli interact with taste substances dissolved in saliva and mucus. 7
The muscles of the tongue are divided into two main groups: intrinsic, which originate and terminate within the tongue, and extrinsic, which originate from structures outside the tongue. The origins of the genioglossus muscle are on the chin, the hyoglossus on the hyoid bone, the palatoglossus in palate mouth, And styloglossus on process styloid. These extrinsic muscles of the tongue move the tongue in the intricate and complex movement patterns necessary for speech. They are also responsible for the movement food in in mouth moment You swallow. Temporary That, The intrinsic muscles of the tongue, which are located entirely within the tongue, help support the activity This. Nerve cranial the 12th, that is nerve hypoglossal (XII), innervate all muscles of the tongue, both intrinsic and extrinsic, except the palatoglossus muscle. This muscle receives innervation from the 10th cranial nerve, namely the vagus nerve (X). 8
Table 1. Muscle On Tongue. . 8

The blood supply to the tongue is derived mainly from the lingual artery, a branch of the external carotid artery. Venous drainage is by the lingual vein. The lingual artery arises from the external carotid artery at the tip of the greater horn of the hyoid bone, in between artery thyroid face And superior. After branching from artery external carotid , the lingual artery runs deep to the hyoglossus muscle and superficial to the middle pharyngeal constrictor muscle. Then, this artery gives rise to the following four arteries: 9,10
The suprahyoid arteries supply the omohyoid, sternothyroid, and thyroid muscles. They anastomose with the corresponding vessels of the opposite side.
The dorsal lingual artery arises beneath the hyoglossus muscle and courses down the back of the dorsum of the tongue. It supplies the mucous membrane in this area as well as the glossopalatine arch, lingual tonsil, soft palate, and epiglottis. It also anastomoses with opposing vessels .
The sublingual artery branches at the anterior border of the hyoglossus muscle before passing between muscle genioglossus And muscle mylohyoid to gland sublingual. Artery This supply gland sublingual before give branch to mylohyoid muscle. This artery also supplies the genioglossus, geniohyoid, and gingival mucosa of the mandible. A branch of the sublingual artery passes posterior to the alveolar process of the mandible and anastomoses with artery Which in accordance in side Which other. Branch second from the sublingual artery pierces the mylohyoid muscle and anastomoses with the submental branch of the facial artery.
The deep lingual artery, which is the end of the lingual artery, passes between the genioglossus muscle and the inferior longitudinal muscle, supplying the upper part of the tongue. The lymphatic vessels of the body of the tongue are divided into the marginal And central. Vessels marginal flow apex tongue, marginal surfaces, and sublingual areas to the submental and submandibular nodes. Less commonly, these vessels drain into the jugulodigastric or jugulo-omohyoid nodes. The central vessels are located at the tip of the tongue, running through muscle mylohyoid, and flow to node jugulo- omohyoid or jugulodigastric. The dorsal vessels collect lymphatic drainage. from area posterior sulcus And flow to node jugulo-omohyoid and jugulodigastric
Lymphatic drainage of the tongue involves multiple pathways. Research has identified various collector vessels lymphatic in tongue, like septum
lingual, deep lingual artery, and superior longitudinal muscle that include lymphatic collections. These vessels drain into different regional lymph nodes, including the submandibular, submental, and subdigastric nodes. In addition, the presence of intraglandular nodes in the parotid gland and lingual lymph nodes for the sublingual gland further contribute to pattern drainage lymphatic Which complex in area head And neck. Understanding these drainage pathways is critical to clinical management, as it can aid in diagnosing metastases and planning surgical intervention for conditions such as carcinoma of the tongue. 11
SCC tongue
Definition
Tongue, together with lips And base mouth, often become subsite which is most frequently involved in the oral cavity. It is important to recognize that although the anterior two-thirds of the tongue is considered part of the oral cavity, the posterior third (base of the tongue) is considered a subsite of the oropharynx. Although histologically similar to conventional oral tongue carcinomas, base of the tongue malignancies have certain implications that distinguish them as disease entities, particularly in terms of treatment, prognosis, and follow-up. Despite advances in the diagnosis and management of oral cancer in recent decades, the long-term prognosis of patients with advanced tongue SCC is generally poor, with a 5-year survival rate of approximately 50%. 12,13
Imaging is necessary to characterize, stage the disease, and assess the relationship of the tumor to surrounding structures. The cervical lymph nodes are also evaluated radiologically, since local spread of the tumor through the lymphatic system, especially to the submandibular and jugulodigastric chains, is common. Therapy is tailored to each patient and, in general, consists of surgery, with chemoradiation also having an important role in selected patients. The goal of therapy is complete cure. while maintain or restore function. Action carry on term
long very important, Because relapse disease in a way local No is rare and should be treated promptly. 12,13
Epidemiology
Neoplasm malignant on tongue tend more often happen on man than women (66-95% of cases), which is in line with the general trend in other parts of the oral cavity. The incidence by sex varies depending on anatomy and has changed with the increase in the number of female smokers. Currently, the male to female ratio is 3:1. Oral cavity and tongue cancers tend to increase with age, especially after the age of 50 years. Most patients develop these cancers between the ages of 50 and 70 years, but they are not uncommon at a younger age. 2,3,14
There are significant differences in the incidence of oral cancer between different geographic regions. The highest incidence of the disease is often found in Asia, which is believed to reflect the prevalence of certain risk factors such as betel quid chewing and smokeless tobacco (snuff) use. In the United States, the incidence is high in urban areas, especially among men, allegedly due to by exposure tobacco And alcohol. Temporary That, Among women in rural areas of the United States, an increased risk of oral cancer is associated with smokeless tobacco use.2,3,14
Etiology And Risk Factors
One of the most significant risk factors for the development of squamous cell carcinoma (SCC) of the tongue is tobacco use. Smoking cigarettes, cigars, and chewing tobacco is a major risk factor for all types of head and neck cancers, including tongue cancer. Eighty-five percent (85%) of head and neck cancer cases are associated with tobacco use. tobacco. Exposure passive to smoke cigarette Also can increases a person's risk of developing head and neck cancer. Based on epidemiological studies, cigar smoking has been shown to be a major risk factor for tumors. cavity mouth, with the only one difference between smoke cigar And conventional cigarettes is the anatomical location where the tumors arise. 2 Smokeless tobacco use has also been associated with an increased incidence of oral cavity cancer. 2 Chewing tobacco is a major cause of oral cancer. squamous mouth And oropharynx in a number of region like India, Asia Southeast, China, and Taiwan, especially when consumed together with betel quid containing areca nut. Although alcohol in itself is a risk factor for the development of cancer of the tongue and oral cavity, its carcinogenic power is less than tobacco. However, when used simultaneously with tobacco, these risk factors become synergistic and result in a significant increase in risk, namely 30 to 36 times for individuals who smoke and consume alcohol simultaneously. In addition, poor oral hygiene and irregular habits in caring for the mouth can also increase the risk of oral cancer. The use of mouthwash containing high alcohol content Also regarded as factor risk potential For cancer tongue and oral cavity (although Not yet proven in a way direct) . Consumption drink like tea and mate (which are commonly consumed by South American people) have been associated with an increased risk of developing oral cavity cancer. Epidemiological studies have shown that intake of vitamin A, β-carotene, and α-tocopherol may reduce risk caught cancer cavity mouth. Besides That, Certain syndromes caused by mutations in certain genes also carry a high risk. caught cancer mouth And tongue. For example is syndrome anemia Fanconi, a disease caused by inherited defects in several genes involved in DNA repair. People with this syndrome often develop hematologic problems at an early age, which can increase their risk of developing leukemia or aplastic anemia. They also have a higher risk of developing oral cancer, especially tongue cancer. Dyskeratosis congenital is also a genetic syndrome that can cause aplastic anemia, skin rash, and abnormality nail on hand And foot; sufferer syndrome This Also own higher risk of developing oral cancer. 3
Diagnosis
The risk factors mentioned in the etiology section of this paper, such as a history of tobacco and alcohol use, should be carefully assessed during the history taking. Any adult patient with symptoms lasting more than two weeks in the upper gastrointestinal tract or without symptoms of a neck tumor should undergo a thorough workup with a high degree of suspicion for malignancy. 2
Physical examination is the best method to detect lesions in the upper aero gastrointestinal tract. Often, the initial assessment also indicates the severity and chronicity of the disease. Because the primary tumor often accompanies cancer head And neck on patient (around 5%), evaluation comprehensive from the entire upper digestive tract is required during diagnosis. Tongue cancer usually causes symptoms that related with the upper gastrointestinal tract, including difficulty swallowing, speaking, hearing, and breathing. During the examination, doctor must focus on symptom like painful tongue, ulcer that do not resolve, and changes in word formation. A complete physical examination should be performed on each patient with special emphasis on examination of the head and neck (including inspection, palpation, otoscopic examination, laryngoscopy No direct, And nasopharyngolaryngoscopy If indicated), and neurological examination with a focus on cranial nerves V to XII. The most common complaint in patients with tongue tumors is pain or a lump. Cancerous tongue mucosa can appear as an ulcer with raised edges or as an exophytic growth. Bleeding from the surface lesi is sign ferocity and must quick cause suspicion of a neoplastic process. 2

Picture 4. Ulceration On Tongue.
Around one third patient sigh about lump in neck. Biopsy lesi tongue often time can done know as procedure take care road depends on anatomical location And preference patient. Biopsy must taken from edge lesions, avoid from areas of necrosis or excessive keratinization. Fine needle aspiration (FNA) is the diagnostic modality Which useful For differentiate gland sap clear benign And fierce in neck. Needle gauge fine make a number of track in on lesi while continue to apply suction. Suction must be released before removing the needle from the lesion. Procedure This own level error negative false as big as 7%. Cytology is very useful in differentiating SCC metastases from other malignant histologies. However, results negative No may interpreted as "No existence disease" when clinically highly suspicious for malignancy. Core needle biopsy should not be performed on neck lumps, except in cases of diagnosed lymphoma. Biopsy gland sap clear excision No only No useful but Also potentially dangerous as a first step in the diagnosis of cancer. A biopsy should be performed only if the diagnosis has not been established after a comprehensive clinical evaluation and at least two non-diagnostic FNA examinations. The surgeon Which do biopsy open must Ready For do maintenance definitive surgery at that time, which may include a formal neck dissection if the diagnosis is SCC. Computed tomography (CT) may be test Which most informative in evaluation tumor cavity mouth And tongue. This can help determine level disease And existence as well as its vastness lymph node involvement. CT has high spatial resolution, allowing to differentiate between fat, muscle, bone, and other soft tissues. CT exceed imaging resonance magnetic (MRI) in detect bone erosion and has a sensitivity of 100% and a specificity of 85%. MRI can provide information Which accurate about size, location, And its vastness tumor involvement in soft tissues. However, MRI is not as good as CT in detecting bony extension unless there is complete involvement of the medullary cavity. Although it has higher sensitivity, MRI has lower specificity than CT. Positron emission tomography (PET) has been evaluated for primary and recurrent carcinomas of the head and neck. 2
More than 90% of head and neck cancers, including oral cavity tumors, are squamous cell carcinomas (SCC). The World Health Organization classifies head and neck SCC into several histologic subtypes, which different, that is: 1. Conventional 2. Verrucous 3. Basaloid 4. Papillary 5. Cell
Spindle (Sarcomatoid) 6. Acantholytic 7. Adenosquamous 8. Cuniculatum Each Variants This Possible develop in various area head And neck, except for the subtype Cuniculatum, Which only found in the layer oral cavity. Variants SCCs frequently arise in the mucosa of the upper aero-gastrointestinal tract, accounting for up to 15% of SCCs in that area. The most common variants include verrucous, exophytic or papillary, spindle cell (sarcomatoid), basaloid, and adenosquamous carcinomas. Every Variants This own characteristics histomorphology Which unique, requiring different differential diagnostic considerations, with implications for appropriate clinical management. Although these SCC subtypes have similar prognoses and management, their histologic stage is not always a consistent predictor of clinical behavior. Characteristics that predict behavior aggressive including infiltration perineural, invasion lymphatic, And expansion tumor outside the lymph node capsule. The Broder grading system is the first quantitative system for cancer. This classification system takes into account the ratio of differentiated to undifferentiated elements in the tumor. There are four histologic grades based on the amount of keratinization: 2
Tumor differentiate Good: > 75% keratinization.
Tumor moderately differentiated: 50-75% keratinization.
Tumor Which differentiate bad: 25-50% keratinization.
Tumor anaplastic or No differentiate: < 25% keratinization.
Immunohistochemical studies may be useful in the diagnosis of poorly differentiated lesions, as SCC expresses epithelial markers such as cytokeratins. Squamous lesions often show positive immunostaining for cytokeratin certain like AE1/AE3 And pancytokeratin. Marker others such as CK5/CK6 and p63 are also useful for squamous differentiation.
Stadium (AJCC 2017 Edition 8 Oral Cavity)
The TNM classification for malignant tumors is the most widely used system for cancer staging in the United States and internationally. This system not only serves as a common language among providers from different specialties who collaborate in the multidisciplinary care of cancer patients, but also guide management And provide prognosis based on population data. The most recent eighth edition of the AJCC Cancer Management Guidelines has presented significant changes. The incorporation of DOI (Depth of Invasion) into the T staging of OSCC (Oral Squamous Cell Carcinoma) is a significant advancement and may it is said late in system TNM from Which recently This published eighth edition. Tumor growth pattern and overall tumor dimensions are increasingly recognized as important features for assessing tumor behavior and determining management local Which optimal. Oncology surgery has long recognized, albeit anecdotally, that small but highly invasive endophytic tumors often signal a much more aggressive clinical and biologic course than with tumor Which very big with expansion Which more to outside the exophytic growth pattern. By incorporating DOI into the routine T staging of OSCC, DOI has been distinguished from other histologic measurements, such as “tumor thickness,” which has long been used inappropriately as an interchangeable term for DOI. In response, the AJCC has issued Instructions explicit For measure DOI in edition eighth AJCC Cancer Management Manual. Microscopic DOI measurements should begin at a horizontal line in the basal layer of the nearest histologically normal-appearing squamous epithelium adjacent to the tumor and extend along the line. upright straight to point deepest invasion tumor. Distance Which measured to point The deepest point on the perpendicular line is the pathologic DOI of the tumor. DOI is distinct from tumor thickness, which is the maximum dimension of the tumor at a given point, regardless of the relationship of the tumor to adjacent uninvolved epithelium. The eighth edition of the AJCC staging system incorporates both clinical and pathologic DOIs. to in stadium T OSCC. Accurate stadium clinical Which accurate relies on physical examination by palpation of the primary tumor and surrounding tissues for induration or fixation to underlying structures indicating a deeper invasive growth pattern. For tumors close to bone, preoperative imaging studies should be performed carefully for signs of bone erosion indicating an invasive growth pattern (T4a). In the updated eighth edition, the DOI for T stage OSCC is classified in 5 mm increments. Less invasive tumors are classified by a DOI of less than or equal to 5 mm, moderately invasive tumors are classified by a DOI of greater than 5 mm and less than or equal to 10 mm, and highly invasive tumors are classified as a DOI of greater than 10 mm. By stratifying for DOI in the eighth edition, tumors with increasing DOI levels were raised from the previous edition which considered only tumor size in determining T stage for OSCC. For example, a 1.5 cm tumor with a DOI of 4 mm is stage T1; whereas a 1.5 cm tumor with a DOI of 6 mm is now stage T2. The staging according to the eighth edition thus distinguishes different stages for 2 tumors that would have been given the same in the seventh edition. Although the incorporation of DOIs into the eighth edition for T staging results in a slightly more complicated system, examination of the data from the eighth edition criteria management T has show discrimination danger which was better in overall survival among patients who had previously treated For OSCC. With thus, patient with tumor Which more invasive have a worse prognosis compared to patients with tumor primary Which size The same but own DOI Which more low, which was previously poorly understood by the seventh edition criteria.15,16
Table 2. Changes from edition seventh to edition eighth Manual Management AJCC Cancer: Category T for oral squamous cell carcinoma. 15

Management
The National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines for head and neck cancer were updated in February 2018. As in edition previously, surgery still become choice main in OSCC treatment. Although therapy primary with radiotherapy single or simultaneously with chemotherapy (chemo-RT) has increase management carcinoma cell squamous outside cavity mouth, surgery still become the basis from the approach curative in management of OSCC. This is due to the ability of surgical resection to address OSCC at all stages, including early and advanced stages. With advances in modern microvascular reconstruction, OSCC patients can undergo simultaneous tumor ablation and reconstruction with optimal functional and cosmetic outcomes. For early-stage disease, a single surgery may suffice, avoiding adjuvant radiotherapy with the risk of long-term residual symptoms. long And morbidity related. However, For part big patient with intermediate to advanced disease, single adjuvant radiation or chemoradiation is recommended to reduce the risk of local and regional recurrence. The role of adjuvant therapy in the treatment of OSCC depends on the pathological T and N stage after resection of the primary tumor and cervical lymph node dissection to reduce the risk of metastasis. Radiotherapy alone or in combination with chemotherapy is recommended as adjuvant therapy for disease on stage carry on, especially when there is feature pathological Which detrimental or metastatic regional nodal pathologically identified. Indications for therapy adjuvan has remained relatively consistent in the 2018 NCCN management guidelines update and should become standard practice for surgeons. 17
Table 3. Indication therapy adjuvant For cancer cavity mouth based on 2018
National Comprehensive Cancer Network . 13

The tongue, especially its anterior two-thirds, is the most common subsite for origin of carcinoma squamous cells in the cavity mouth. Thing this is because tongue considered as subsite at risk tall For OSCC Because tend For metastasis nodal regional through network lymphatic Which rich and resistance Which low to invasion tumor And metastasis. Management main and definitive treatment of OSCC of the tongue, with curative intent, generally involves surgery alone or in combination with adjuvant radiation or chemo-RT, as indicated by pathological stage. The choice of reconstruction after tongue resection depends on the size of the defect after ablation, the overall functional status patient, need For modality treatment addition, And the hope of maintaining tongue function, including speech, chewing, and swallowing. reconstructive, defect small on tongue can overcome with primary closure; medium-sized defects with skin grafts or biological dressings; while large partial glossectomy, hemiglossectomy, and subtotal or total glossectomy is better done with use flap local (for example, myomucosa artery face and submental flaps) or free tissue transfers (eg, radial forearm flap, flap thigh anterolateral, flap arm lateral, flap artery sural medial perforator, and deep perforator artery flap). The management of early stage T1-T2 OSCC of the tongue with a negative neck (cN0) remains a controversial topic in surgical oncology. Due to the possibility of occult metastases in OSCC of the tongue at presentation, many surgeons recommend elective nodal dissection (END) even for early stage (T-stage) cancers with the aim of to obtain information prognostic of identification node regional on during surgery. Although a number of variation in recommendation expert surgery For END in early stage T tongue cancer, evidence suggests that most recommend END for patients with stage cT2 or greater tongue tumors. This practice pattern is now considered in light of updates to the AJCC Cancer Staging Manual and NCCN Guidelines, which recommend management based on threshold limit objective from depth of primary invasion (DOI) at the primary site to estimate the risk of occult nodal metastases. However, although the NCCN currently recommends a DOI threshold of 4 mm as the inflection point for considering END for OSCC, this recommendation does not account for specific risks by subsite anatomy tumor primary in cavity mouth. Study latest show that for high-risk anatomical subsites in the oral cavity, the DOI threshold Which more low (2 mm For tongue And 2-3 mm For floor mouth) may be more appropriate to recommend END. Nevertheless, most surgeons still consider the 4 mm threshold for DOI as the criterion for recommending END in cases of early stage cN0 tongue carcinoma because risk Which significant from metastasis nodal hidden on moment diagnosis. Sentinel biopsy (SNB) remains a viable alternative in the management of early-stage cN0 tongue cancer, especially when preoperative DOI assessment is No available or No clear. Tumor tongue Which spread to floor The mouth, however, is less suitable for the SNB technique.4,13
The mobile tongue can be divided into three segments. The anterior and middle segments are separated by the median raphe, which serves as a natural barrier to tumor spread. Meanwhile, the base of the tongue includes one third part behind tongue, including papilla circular And lymphatic tissue. The new classification system for tongue disorders focuses on functional subunits Which need reconstruction. This based on on findings defect intraoperative tongue, Which we classify become five group based on reconstruction complexity level: 18
Type 1 defect: unilateral and marginal defect, rarely involving the tip of the tongue without pass line middle, No expand to more from one third part tongue that moves and does not involve the back third of the tongue.
Type 2 defect: unilateral defect that does not cross the midline without involvement of the posterior third, but extends to more than one third of the tongue.
Type 3 defect: the defect involves the anterior two-thirds of the body of the tongue moving with contralateral extension.
Type 4 defect: involves the base of the tongue, with variant 4A involving less than 50% of the base of the tongue and variant 4B involving more than 50% of the base of the tongue.
Type 5 defects: any type of defect involving the floor of the mouth, with or without bone resection.
Choice technique reconstruction in algorithm determined by estimation
volume tongue Which will replaced, with objective return form And natural volume of the tongue and maintaining remaining mobility for good functional results. In this system, type 1 and 2 defects primarily require restoration of the shape tongue Because more from 50% body tongue Which move can maintained with good functional expectations. On the other hand, type 3 and 4 defects require extensive tongue resection, resulting in complex tissue loss. In cases this, more of 50% of the entire body of the tongue needs to be replaced, with a decrease significant in function swallow And speak on case resection base broad tongue (type 4B). 18

Picture 5. Representation schematic from three segment body tongue, each divided in throughout median tongue raphe
Prognosis
Historically, SCC of the tongue in young adults has been considered by many authors to be a highly aggressive clinical entity, with a high risk of local-regional recurrence, and a lower survival rate than the general population and resulting in the need for more aggressive therapy. However, considering the majority of studies latest, results prognostic on patient group it is heterogeneous and it is not possible to confirm this trend. The heterogeneity of these results may also depend on the definition of the variable "young age", with a wide range of age limits ranging from 30 to 45 years. In the future, to make the data more homogeneous And can compared to, has recommended that Possible It would be useful to consider young patients only those under 30 years of age. In the specific field of SCC of the tongue, an analysis of a case series of 276 patients (66 under and 210 over the age of 45) conducted by Knopf and colleagues has disclose profit prognostic Which significant on the patient who more young. Regardless from consideration This, very important For interpreting these results is likely influenced by tumor extension, and thus T category, which was significantly lower in patients under 45 years (with no difference in N category and M). categories N and M). This selection bias is partly mitigated by matched case studies characterized by a homogeneous distribution of patients with regard to tumor characteristics and comorbidities. On the other hand, several studies have shown no prognostically significant differences, taking into account 87 patient aged ≤ 45 year in A studies by Lassig and colleagues 44 and 31 patients ≤ 40 years of age analyzed by Pytynia and colleagues 45, both of which were matched cases and included head and neck tumors in general. general. Trends Which No significant to prognosis Which more bad has also been reported by a group led by Kourelis 50 who considered only patients with SCC tongue stadium beginning. In particular, in young women, there was also evidence of a significant increase in the risk of recurrence compared with Recommendations for follow-up based on the risk of recurrence, second primaries, residual symptoms of treatment, and toxicity include history and physical examination (including head and neck examination) complete; laryngoscopy And fiber optics like Which indicated in a way clinically every 1 to 3 months for the first year, every 2-6 months for the second year, every 4 to 8 month on 3rd year up to the 5th, and every 12 months after 5 years. To facilitate this, our group sees patients quarterly for the first 5 years. Posttreatment baseline imaging of the primary (and neck, if treated) is recommended within 6 months of treatment, with imaging thereafter indicated based on signs and symptoms (but not routinely recommended without worrisome manifestations). Chest imaging as clinically indicated for patients with a history of smoking. If the neck is radiated, NCCN guidelines recommend thyroid stimulating hormone (TSH) every 6 to 12 months. Smoking and alcohol counseling as clinically indicated. 3,13
Mandibulotomy
Definition
Mandibulotomy is a surgical approach used to access and perform resection of tumors in the oral cavity, oropharynx, and parapharyngeal space. Various techniques have been developed to perform mandibulotomy, such as paramedian lateral angle mandibulotomy to reduce side injuries. This procedure involves mandibular osteotomy to provide adequate exposure for tumor removal, with different designs tailored to specific anatomical conditions. 19,20
History
Mandibulotomy is essential to gain access to the parapharyngeal region, which is attached laterally by the mandibular ramus and condyle. Roux on at first describe mandibulotomy or swing mandible in historical term in 1836. Dubner and Spiro later described a modified mandibulotomy and paralingual extension in 1959. Each strategy has its own advantages and disadvantages; in a study, Riddle et a. until on conclusion that complaint main in midline mandibular osteotomy is malocclusion. Papadogeorgakis and colleagues provide five criteria for selecting the most effective strategy, namely:
1. Connection tumor And structure neurovascular. 2. Dimensions tumor. 3. Tumor vascularization. 4. Proximity of the lesion to the pharyngeal wall. 5. Malignant potential. Mandibulotomy described in the literature has advantages and disadvantages . 19,20
Mandibulotomy has evolved as a surgical approach for a variety of conditions in the oral cavity and oropharynx. technique has developed to optimize results and minimize complications. Approach Midline mandibulotomy has been widely used for oral and oropharyngeal tumors, providing excellent exposure with a lower complication rate than with approach posterior . Besides That, technique mandibulotomy modified has been introduced for resection of parapharyngeal space tumors, ensuring complete tumor removal while preserving mandibular integrity and functionality. Furthermore, a paramedian lateral angle mandibulotomy design has been proposed to reduce side injuries during compartmental resection of squamous cell carcinoma in the oral cavity, emphasizing the importance of considering condition anatomy local For prevent complications. These advances highlight the ongoing refinement and adaptation of mandibulotomy techniques to improve surgical outcomes.19,20
Operation Technique
The submandibular incision is placed in the skin crease around the chin and on the lower lip in a ladder pattern. The subplatysmal flap is elevated, and supraomohyoid neck dissection is performed with clearance up to level III. Then, the incision is extended intraorally along the labial mucosa to the mucoperiosteum. mandible, with incision interdental placed in between canine tooth And tooth premolar First, Which Far from location osteotomy. Mucoperiosteum. lingually reflected after placing the crevicular incision up to the last molar tooth still standing in the oral cavity and extended buccally. The osteotomy was planned anterior to the mental foramen between the canine and first premolar teeth in a stepwise manner using a straight fissure bur followed by a saw. The osteotomy was then completed using an osteotome. Initial plating of the osteotomized segment was performed to achieve accurate anatomical reduction and to prevent asymmetry. The mandibulotomy segment was separated from the lingual mucoperiosteum during elevation. Lingual nerve identified And preserved. Fiber muscle pterygoid medial stripped from medial aspect of the mandible, and the inferior alveolar neurovascular bundle are identified and preserved. Stripping of the temporalis muscle fibers is performed from the coronoid process along with release of the stylomandibular ligament from the ramal area of the mandible to achieve lateral swing of the mandible for adequate exposure. A maxillary degloving incision is performed for lesions requiring maxillectomy (partial, total). The lateral nasal wall, frontal process of the maxilla, zygoma, And edge orbita exposed. Transfascial approach expanded used for lesions extending to the medial orbital wall for orbital exenteration. Maxillectomy is performed partially or completely depending on the extent of the lesion. Yes block resection tumor done together with cleaning from area infratemporal fossa. Resection was followed by reconstruction using temporalis myofascial flap, forehead flap, and spilled thickness graft with obturator. Mandibular fixation was performed using 2 miniplates followed by intraoral and extraoral closure along with placement of drains in the neck and temporal region. 21
Lateral mandibulotomy, in which an incision is made posterior to the mental foramen during the mandibulotomy procedure, has certain disadvantages. One of the disadvantages is is the occurrence denervation on teeth distal And devascularization of the blood supply mandible because piece located in behind foramen mental. This is caused by different directions of muscle pull, causing delays. in recovery. Delay healing This occurs especially in the field area when postoperative radiation is intended. Midline mandibulotomy, in where tooth series middle must removed Because cutting line middle, has a negative cosmetic impact. In addition, this procedure causes disruption of the floor of the mouth while cutting the geniohyoid and genioglossus muscles, which can delay the recovery process in swallowing. Paramedian mandibulotomy, in which the mental nerve and blood vessels are preserved during the cut is performed between the lateral incisors and canines, i.e. anterior to the mental foramen, but involves violation of the lateral part of the mouth involving the mylohyoid muscle, which in turn can also delay the recovery process. 19,20
Surgical approaches to tongue cancer resection vary widely, and the optimal approach remains an open question. However, the anesthetic and functional outcomes of lip surgery are controversial. This study used the following approach: Modified Supraomohyoid Mandibulotomy (MSMM) Which different of the previous non-lip-splitting approach for oncological resection and defect reconstruction in different stages of TSCC. The aim of this retrospective paired cohort study was to assess tumor recurrence, functional, and aesthetic outcomes of the MSMM approach versus the Lip Splitting Mandibulotomy approach. (NGO). Approach surgery Which appropriate very important For extensive tongue tumor resection, and R0 block resection further affects the patient's prognosis. Clinical application of the non-lip-splitting approach for patients with TSCC Not yet accepted in a way wide by for expert surgery Because concerns about inadequate tumor exposure. However, some surgeons consider this approach effective in achieving good tumor control and satisfactory aesthetic results. The MSMM approach in this study is different from previous non-lip-splitting approaches. First, the lip incision is moved to the submental area to increase the width of the protective flap and expose the mandible. Second, mandibulotomy can be performed easily with this approach. Third, semi-tongue splitting is performed before mandibulotomy to obtain optimal tumor exposure and negative margins. This study showed similar tumor recurrence and prognosis of patients with TSCC between the MSMM and LSM approaches. Thus, the MSMM approach without lip splitting is safe for oncological resection of patients with TSCC. Mandibulotomy in maintenance surgery cancer mouth And oropharyngeal is still controversial. Tumor control and frequency of complications associated with this procedure vary in many studies. The mandibular preservation approach has shown a lower complication rate after surgery. However, other studies have shown that the mandibulotomy approach provides better local control and better disease-free survival. compared to with resection transoral without mandibulotomy on cancer tongue pT2.5
Complications
Complications Which related with mandibulotomy covering osteoradionecrosis, fistula formation, malunion, surgical site infection, and plate exposure. Regardless from potential complications, mandibulotomy still become tool Which valuable in head and neck surgery, offering a safe and effective means of tumor resection. while guard integrity And functionality mandible. 19,20 On Min et al.'s study, the rate of fistula complications and osteoradionecrosis low mandible, and adequate soft tissue coverage with free flap and fixation reliable important For prevention complications after operation. Results aesthetics and functional and other QOL domains were superior through the MSMM approach without lip division based on the POSAS and UW-QOL results in this study. However, other studies concluded that there was no significant difference in scarring and self-perception between the non-lip division and lip division approaches. This suggests that both approaches provide satisfactory outcomes for oral cancer patients after surgery. 5
Flap Myocutaneous Pectoralis Major
Definition
The first report of the pectoralis major muscle flap (PMMF) appeared in the literature in 1968 by Dr. Hueston, a surgeon from Melbourne, Australia. In the report, he described the fusion of the pectoralis major muscle with skin in above it For reconstruct disabled wall chest. Around One decade Then, on year 1979, description PMMF For reconstruction head and neck were described separately by Ariyan and Baek. This stems in part from Conley's earlier work introducing the deltopectoral flap for reconstruction of head and neck defects. Although microvascular free tissue transfer has become the mainstay for patients with complex head and neck reconstruction, a good understanding of PMMF remains essential for primary reconstruction, rescue, and emergency procedures. However, role PMMF still not replaced especially on patient at risk high, vascularized neck, and in surgical candidates who are less suitable for total free tissue transfer.22
Technique
Pectoralis major is muscle superficial big Which protruding go out from middle part clavicle, elongated until bone vulnerable costa second until seventh and the aponeurosis of the external oblique muscle. The muscle fibers then unite laterally to enter to in tubercle Which more big from humerus. Pedicle vascular, consisting of the pectoral branch of the thoracoacromial artery and its accompanying vein, lies on the undersurface of the muscle, adjacent to the pectoralis minor and costal cartilages. The lateral thoracic artery serves as a secondary blood supply to muscle pectoralis major And often time tied up For reach rotation and long Which optimal. Nerves motor main muscle pectoralis major originate from the lateral branches of the pectoral nerves arising from the brachial plexus (C5-C7). The vascular pedicle can be easily identified on the undersurface of the pectoralis major muscle and can be predicted using well-established techniques. Use technique This very help in plan closing skin and ensure that the vascular pedicle is properly inserted into the flap. Design and elevation flap skin For use in reconstruction depends on defect what is needed closed, with every part skin in on muscle pectoralis still useful in flap design. The medial aspect of the pectoralis major inserts into the second to sixth costal cartilages. The incision design for the PMMC flap must take into account the exact anatomical location and consider aesthetic aspects. There are several ways For to organize incision For flap PMMC, with concepts certain Which allows early identification of the pectoralis major muscle and vascular pedicle and intraoperative design modification as needed. The length of the pedicle can be estimated by measuring the distance between the superior border of the skin paddle and the inferior border of the clavicle, which should approximate the distance between the defect and the inferior border of the clavicle. The incision for the PMMC flap requires careful consideration, especially in considering the nipple areolar complex. The use of fresh cadavers has helped understand the contribution of the nipple areolar complex to the blood supply to the PMMC flap. Inclusion of the nipple areolar complex may affect esthetics and patient satisfaction, and thorough discussion with the patient is necessary. There is evidence that including the nipple areolar complex in the PMMC flap can provide good results without significant skin flap loss. However, complications associated with this procedure must be carefully considered in surgical planning. 22
Based on planning incision Which outlined on Picture 2, The initial approach is from lateral to medial, starting from the humerus towards the second costal cartilage. This incision is made using a Bovie electrocautery on a cutting setting through the skin with care to identify the underlying pectoralis major muscle. The incision is then carried medially along the sternum and inferiorly according to the patient's reconstruction needs, taking care not to cut the pectoralis muscle prematurely. At this stage, the superior, medial, and inferior lines of the PMMC flap have been defined, and the pectoralis major muscle is freed medially from the sternum and inferiorly from the chest wall. The breast perforators adjacent to the sternum that supply the deltopectoral flap are also identified and inadvertent ligation of these vessels must be avoided, which is important for the patient Which Possible requires a deltopectoral flap in time front. Anchoring stitches sometimes placed moment This or after finished all skin incision to prevent shear. The muscle flap is then lifted from the chest wall beneath the pectoralis major muscle fascia. Bleeding from chest wall perforators is common And controlled with clip vascular, bipolar, or electrocautery bovie. Ligation of blood vessels is very important because these blood vessels will retract and can lead to hemothorax if not treated when first discovered. After field intermuscular identified between muscle pectoralis major and minor, one can easily free the pectoralis major and its vascular pedicle (which runs on the undersurface) from the pectoralis minor using dissection blunt. On point This, incision lateral on paddle skin created if not already done. Waiting to slice lateral skin paddle at this point allows modification on closing skin For ensure pedicle blood vessel entered with Good. After paddle skin sliced fully, skin sutured to the muscle and fascia to prevent sliding of the skin paddle from the anterior surface of the muscle. Using the PMMC flap in the non-dominant hand, the pectoralis muscle released in a manner lateral by keeping pedicle still seen. Branch of artery thoracic lateral And nerve pectoralis medial shared with using vascular clips to avoid thermal injury to the pedicle. Tunneling between the neck and chest is performed at a later stage. The weakening wide between skin And aspect superior muscle pectoralis done For create a skin/fascial tunnel between the chest and neck, taking care to preserve the perforators to the overlying deltopectoral. A large retractor is placed in neck in on clavicle For facilitate entry tool from chest to neck, with a minimum of 3-4 the finger that must be easily pass through tunnel to ensure the opening is wide enough to accommodate the PMMC flap which is then passed through the tunnel into the neck. If additional length is required, an incision into the clavicle and pectoralis major muscle can be made, taking care to keep the pedicle in view at all times to provide increased mobility. Insertion, closure, and monitoring of the PMMC flap will be determined by demands resection, However principles following This important: Secure sutures should be placed in both the muscle fascia and skin within the inset to help distribute the weight of the flap and prevent pulling on the skin paddle. Care should be taken to ensure that previously removed sutures do not interfere with the inset, especially in the setting of pharyngeal reconstruction after laryngectomy. total. Hemostasis on location donor chest must checked And irrigated, with two channel suck closed ideally placed in in chest Which Then closed in two layer in accordance with preference doctor surgery. Additional holes may be needed to facilitate chest wall closure, and tension addition Which happen must be noticed And handled. Important to avoid unnecessary pressure on the pedicles around the neck, and to mark location in wall chest place Closing PMMC played with itself can help ensure proper flap inset. 22

Picture 6. Vascular pedicle and.Skin flap elevation.22
REFERENCE
Descendants R. Cancer Facts & Figures 2018. Am Cancer Soc. 2018;233–6.
Arrangoiz R, Cordera F, Caba D, Moreno E, Luque de Leon E, Munoz M. Oral Tongue Cancer: Literature Review and Current Management. Cancer Reports Rev. 2018;2(3):1–9.
Paderno A, Morello R, Piazza C. Tongue carcinoma in young adults: A review of the literature. Acta Otorhinolaryngol Ital. 2018;38(3):175–80.
Leoncini E, Ricciardi W, Cadoni G, Arzani D, Petrelli L, Paludetti G, et al. Adult height and head and neck cancer: A pooled analysis within the INHANCE Consortium. Head Neck. 2014;36(10):1391.
Min F, Qiu P, Zhu X, Zhou B, Lin Z, Pan C, et al. Modified submandibular mandibulotomy approach versus lip-splitting approach in tongue cancer surgery: a retrospective paired-cohort study. Clin Oral Investig. 2024;28(1):1–12.
Setiawan IGB, Pramegia DKNS. Flap selections in the reconstruction of tongue squamous cell carcinoma following glossectomy. Int J Health Sci (Qassim). 2022;6(May):10204–14.
Vinet L, Zhedanov A. Ganong Anatomy and Physiology [Internet]. 2019. Available from: http://jurnal.globalhealthsciencegroup.com/index.php/JPPP/article/downloa d/83/65%0A http://www.embase.com/search/results?subaction=viewrecord &from=export&id=L603546864% 5Cnht tp: //dx.doi.org/10.1155/2015/42072 3%0A http://link.springer.com/10.1007/978-3-319-76
Martini F, Tallitsch RB, Nath JL. Human anatomy / Frederic H. Martini, Ph.D., University of Hawaii at Manoa, Robert B. Tallitsch, Ph.D., Augustana College, Rock Island, IL, Gambling L. Nathan, Ph.D., Lourdes University, Sylvania, OH. Pearson Education. 2018. A6 p.
Buffoli B, The Verzeletti V, Rezzani R, Rodella LF. Unusual branch of the lingual artery supplies the infrahyoid muscles. Anat Sci Int [Internet]. 2020;95(1):153–5. Available from: https://doi.org/10.1007/s12565-019-00501-6
Ary K. Dotiwala. Anatomy, Head and Neck, Tongue. 2023;
Abou-Foul AK. Surgical anatomy of the lymphatic drainage of the salivary glands: A systematic review. J Laryngol Otol. 2020;134(10):856–62.
Mario Gonzalez. Tongue Cancer. 2023;
Ettinger KS, Ganry L, Fernandes RP. Oral Cavity Cancer. Oral Maxillofac Surg Clin North Am [Internet]. 2019;31(1):13–29. Available from: https://doi.org/10.1016/j.coms.2018.08.002
Blanchard P, Belkhir F, Theme S, El Khoury C, With Felicity F, Casiraghi Oh, et al. Outcomes and prognostic factors for squamous cell carcinoma the oral tongue in young adults: a single-institution case-matched analysis. Eur Arch Oto-Rhino-Laryngology. 2017;274(3):1683–90.
Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–9.
Ebrahimi A, Gil Z, Amit M, Yen TC, Liao CT, Chaturvedi P, et al. Primary tumor staging for oral cancer and a proposed modification incorporating depth of invasion: An international multicenter retrospective study. JAMA Otolaryngol - Head Neck Surg. 2014;140(12):1138–48.
Pfister DG, Spencer S, Adelstein D, Adkins D, Brize DM, Burt B. NCCN Clinical Practice Guidelines: Head and Neck Cancer. Version 1.2018. J Natl Comprehensive Cancer Netw. 2018;218.
Mannelli G, Arcuri F, Agostini T, Innocenti M, Raffaini M, Spinelli G. Classification of tongue cancer resection and treatment algorithm. J Surg Oncol. 2018;117(5):1092–9.
Shinghal T, Bissada E, Chan HB, Wood RE, Atenafu EG, Brown DH, et al. Medial Mandibulotomies: Is there sufficient space in the midline to allow a mandibulotomy without compromising the dentition? J Otolaryngol - Head Neck Surg. 2013;42(MAY):1–7.
Singh A, Arora RD, Dange PS, Nagarkar NM, Raghani M. Modified mandibulotomy US an approach to parapharyngeal space tumors: a case report. Egypt J Otolaryngol [Internet]. 2023;39(1):1–5. Available from: https://doi.org/10.1186/s43163-023-00469-1
Anehosur V, Bindal M, Kumar N, Shetty C. Mandibulotomy Approach for Resection of Maxillary Tumours: A Clinical Review. J Maxillofac Oral Surg [Internet]. 2019;18(3):360–5. Available from: https://doi.org/10.1007/s12663-018-1164-6
Watts TL. The pectoralis major myocutaneous flap. Operation Tech Otolaryngol - Head Neck Surg [Internet]. 2019;30(2):134–7. Available from: https://doi.org/10.1016/j.otot.2019.04.008
Shekhar Gogna; Kashyap Nest; Nagendra Gupta. Neck Cancer Resection and Dissection. 2023;
McLean JN, Carlson GW, Lost A. The pectoralis major myocutaneous flap revisited: A reliable technique for head and neck reconstruction. Ann Plast Surg. 2010;64(5):570–3
sdgsd
Comments