LITERATURE REVIEW
I Made Nudi Arthana
1 Definition And Indication Tympanoplasty
Definition Tympanoplasty
Tympanoplasty is a middle ear surgery that aims to repair the middle ear system. aeration from tube eustachian tube until with bone temporal as well as repair the mechanical sound wave delivery system and create clean and dry conditions. This reconstruction operation is often used as one system of reconstructive surgery for the auditory bones or tympano-ossicular system which includes canaloplasty, myringoplasty and ossiculoplasty with the understanding that canaloplasty is an action to widen the auditory canal external, myringoplasty is action For reconstruct tympanic membrane using a graft to cover the tympanic membrane perforation so that it can restore its vibration function and ossiculoplasty is a surgical procedure to reconstruct bone hearing. Tympanoplasty often Also accompany Mastoidectomy, either whole wall mastoidectomy or collapsed wall mastoidectomy, and is usually performed at the end of the mastoidectomy procedure. 1
Reconstruction membrane timpani first time recorded on century 17 when Banzer in 1640 described his attempt to patch a perforated tympanic membrane using a pig's bladder stretched over an ivory funnel. The concept For repair perforation membrane timpani in a way revolutionary introduced by Wullstein and Zollner in 1952 and 1955. The term tympanoplasty was first introduced by Wullstein in 1953 who then divided tympanoplasty into 5 type on year 1959. Wullstein close perforation membrane timpani with split thickness skin graft. Shea on year 1957, when do stapedectomy, get accidentally, the vein wall can to close the tympanic membrane perforation. Then House, Glasscock And Sheehee modify technique That become technique onlay used until Now. Technique underlay First time reported by Shea Which when performing stapedectomy, he accidentally managed to close the torn tympanic membrane using the temporalis muscle fascia and reported a series of successes using the fascia as a graft. 2
Microscopic tympanoplasty has been the standard procedure for effective reconstruction of perforated tympanic membranes since the mid-20th century. This approach has some disadvantages due to the retroauricular incision and the need for canaloplasty, especially in cases of anterior perforations. However, the endoscopic approach is very advantageous in cases of anteriorly located and difficult to see tympanic membrane perforations. In these cases, when the microscopic approach is chosen in institution we, as well as many surgeons otology other Which often choose to perform a retroauricular incision. Since endoscopic ear surgery was first performed in year 1990s, surgery This is branch surgery otology Which Keep going develop and minimum invasive. Endoscopy is tool Which ideal, Which allow doctor surgery to perform a complete transcanal endoscopic ear surgery, whereas the classical microscopic approach would most likely require an additional external incision, or a mastoidectomy.3
Indication Tympanoplasty
The goal of tympanoplasty is to reconstruct the TM with or without reconstruction of the ossicular chain, thereby preventing recurrent infection (otorrhoea) and restoring hearing. The main indications are CSOM or CSOM with cholesteatoma. 12,15 Other indications are
Decrease hearing type conduction Which because of perforation membrane timpani
Otitis media Which chronicle or recurrent Because contamination consequence from tympanic membrane perforation
Perforation drum ear Which settle down more from 3 month
Perforation I healed without treatment on around 80% patient Also can need improvement
Traumatic TM perforation caused by mechanical trauma that does not heal
Discontinuity bone hearing
For fixate bone hearing 1
Contraindications Tympanoplasty
Contraindications For tympanoplasty can categorized become relatively or Absolute contraindications. Relative contraindications include patient age (extremes of age), non-functioning Eustachian tube, dead ear (non-hearing), or consideration of tympanoplasty in the better-hearing ear. Absolute contraindications include uncontrolled cholesteatoma, uncontrolled complications or symptoms. remainder from otitis media like abscess intracranial, meningitis or thrombosis sine lateral, malignancy, or patient-specific anesthetic contraindications . 4
2 Classification Tympanoplasty
There are five basic types of tympanoplasty procedures according to Wullstein (1959) based on the concept of sound transformation in the foramen ovale and sound protection in the foramen rotundum.
Tympanoplasty type I or Which called myringoplasty. Only reconstruct the membrane timpani Which experience perforation without change system bone
hearing. Included in this procedure is exploring the condition of the middle ear and ensuring the condition of the auditory ossicles.
Type II tympanoplasty is used for tympanic membrane perforation with erosion of the malleus. It involves grafting/placement of a graft on the incus or remnant of the malleus. the. The goal is repair membrane timpani And lever mechanism played by malleus and incus. Some of the auditory bones have been damaged, so they are trying to be preserved and reconnected.
Tympanoplasty type III indicated For condition the damage two bone hearing with the stapes still intact and mobile. This involves the placement of a graft to the stapes, aimed at restoring the sound conduction process to the foramen ovale. myringostapediopexy which results in a shallow middle ear and Columella effect.
Type IV tympanoplasty is used for ossicular damage involving all or part of the stapes arch. It involves placing a graft on or around the mobile stapes footplate.
Type V tympanoplasty is used on the fixed stapes footplate. The graft on the fixed stapes is to protect the foramen ovale. 1,2
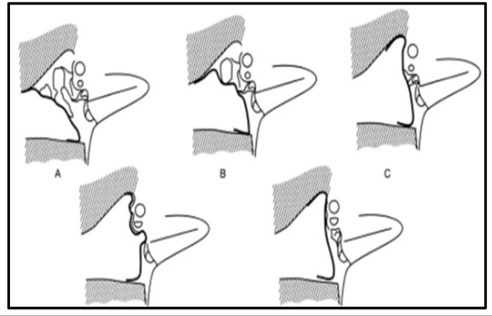
Picture 1 Types Tympanoplasty according to Wullstein
3 Procedure Tympanoplasty
Several types of tissue are used as graft material in tympanoplasty techniques. Starting with Wullstein who used split thickness skin graft and full thickness, to reconstruct tympanic membrane perforation, it turned out not to last long because it experienced desquamation which invited infection and reperforation. Then Mortiz and Zolner who used pedicle flap and Shea used vein wall, the search for material graft This continues to grow until 1961 storrs using fascia temporalis and perfected its technique by Glasscock. Since then the use of fascia specifically temporal fascia the more develop Because material This easy obtained, more sturdy from loose and more elastic connective tissue than the vein wall. In conditions of quite severe middle ear infections, the presence of retraction pockets, atelectasis and impaired tube function, causing the temporal fascia graft to become more prone to atrophy and reperforation so that experts are looking for other stronger materials to prevent reperforation, atrophy and retraction. Then cartilage was found as a substitute for fascia. Cartilage is the most commonly used is originate from tragus And concha. Cartilage tragus straighter so that no need formation return And more easy For taken. On the contrary Concha cartilage, more curved, must be reshaped and the process of taking it is quite difficult, but concha cartilage can be chosen if we need a graft that is quite wide/large. 1 5
There are various cartilage tympanoplasty techniques, but Mirko Tos broadly classifies them into 6 techniques, namely:
Underlay palisade , method Heerman
Onlay palisade
Broad palisade
Underlay stripes
Onlay stripes
Dornhoffer mosaic cartilage tympanoplasty
Tympanoplasty techniques are increasingly day by day develop, the experts trying to find a technique and materials graft Which can give results which is satisfying. On year 2010, Neumann et al. studied 29 patients who underwent cartilage tympanoplasty over a period of more than 9 years. Indication operation on subject study This Because cholesteatoma, otitis media chronic, perforation sub total And timpanic fibrosis. Results from study the show that
no reperforation occurred, total healing was 100%. In the same year, Cabra et al also studied the effectiveness of cartilage tympanoplasty compared to tympanoplasty using graft fascia, with subject study 123 patient. Results from study The results are that in both types of tympanoplasty there is improvement in terms of morphology and hearing function, but the success rate of cartilage tympanoplasty is 84% while fascia tympanoplasty is only 64%. However, there is no difference in the results of the improvement. function hearing. Comparison results end from tympanoplasty cartilage with tympanoplasty fascia too in detail by Onal K et al. on year 2011, and get The success rate for fascia was 65.9% and cartilage 92.3% and cartilage tympanoplasty gave better hearing improvement results than fascia tympanoplasty .
The majority of middle ear surgeries involving the TM are classically performed using the postauricular approach; endaural (through the ear canal) and transcanal approaches are also used. Each technique has advantages and limitations and factors to consider when deciding which approach to use include: size perforation TM, size hole ears, and preference doctor surgery. Like in other surgical fields, the trend is towards more minimal technical direction invasive has made Trans-canal or endoscopic ear surgery is becoming increasingly popular.
Preparation theater standard done let go from technique tympanoplasty Which used. Prophylactic antibiotics are usually given (although not as much during endoscopic surgery). The patient lies supine on the operating table; a head ring is used to provide stability. If necessary, the patient's hair is shaved in the postauricular area. Local infiltration (lidocaine with adrenaline) is given, and local hemostasis should be achieved. The ear canal is inspected and cleaned as necessary, and perforation of the TM and ossicles is assessed under microscopic or endoscopic vision before starting the procedure. 6
Graft
Autologous grafting materials are readily available, biocompatible, and inexpensive; therefore, there is limited rationale for using synthetic alternatives. Autologous grafts are typically made from the temporal fascia or tragal/conchal perichondrium; however, research Also report use fascia lata, skin channel, And periosteum.
The advantages of using alloplastic grafts such as acellular dermal matrix and gelatin sponge Which can absorbed especially covers decrease morbidity Which related with autologous grafting, namely reduced pain and better cosmetic results without additional scarring. However, the cost implications of using this graft and the risk of transmitting infectious diseases may outweigh the above-mentioned advantages. In practice, autologous grafting is the preferred type for use by many otolaryngologists. 7
Most expert surgery use fascia temporalis Which more general used in practice than cartilage, and the success rate of using this graft in tympanoplasty ranges from 93% to 97%. However, in situations that require improvement stability, like perforation repetitive or patient at risk height, bone vulnerable And perichondrium can harvested with make incision through side medial to the tragus skin, perichondrium, and cartilage. Although the use of cartilage has proven more successful than temporalis fascia, largely because its high tensile strength makes it more resistant to shrinkage, there is sometimes doubts about good electrical conductivity. 8
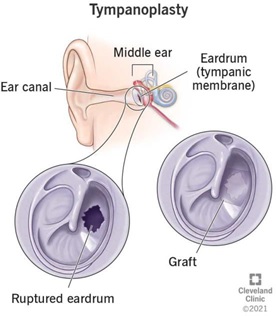
Picture 2 Installation Graft on rupture membrane timpani
Approach with Microscope
When using a microscope, the postauricular and trans-canal approaches are frequently used for tympanoplasty. The Lempert endaural approach is much less frequently used in tympanoplasty modern, but still is choice Which worthy. Procedure This begins with the surgeon making a semicircular incision about 1 cm behind the skin crease of the earlobe; the ear is folded anteriorly. This incision is brought down through the musculoperiosteum For create flap musculoperiosteal, Which elevated toward the membranous ear canal, thus entering the bony ear canal. The skin along the posterior aspect of the bony canal is lifted until the surgeon reaches the tympanic flap incision. The tympanic flap can then be elevated, and the middle ear can be entered.
At this stage, if necessary, the ossicular chain can be repaired by performing an ossicularoplasty. The edges of the TM perforation are refreshed with scissors or cup forceps. Underlay technique, in where limbus is weakened, TM was lifted, and perforation closed with medially, used to reconstruct the TM. For optimal success, the autologous graft should cover the TM defect and also be anchored to the ear canal for stabilization. Care should be taken to avoid damaging the chorda tympani posteriorly when lifting the limbus from its bony sulcus. 9
Approach with Endoscopy
Repair perforation TM in a way endoscopy No too invasive compared to with the traditional postauricular and endaural approaches. This can provide a better view more wide to anatomy ear middle without make incision external, so as to reduce time operation And recovery. Study has show level closure of perforations and similar audiological recovery compared to microscopic tympanoplasty. Disadvantages of endoscopic middle ear surgery include surgical manipulation done with One hand And potential danger Which due to by production heat from the endoscopic light source to the surrounding structures. 1 0
Endoscopic tympanoplasty is performed using a transcanal approach. As previously, edge perforation removed the epithelium necessary. Incision made in ear canal (endoural, circumference lateral, or door swing), Which allow flap tympanomeatal and annulus lifted, so that create access to ear middle. Malleus peeled from TM, And on stage This, chain ossicular fixed (ossiculoplasty) If required. The prepared graft is placed on the medial part of the TM remnant and on the lateral part of the malleus. Gel foam sponges are inserted into the middle and external ear canals. Recently, the 'butterfly cartilage tympanoplasty technique' has been described in the literature, which does not require the tympanic flap to be raised. After creating the pseudo-flange of the bone vulnerable, graft placed to in perforation, with One flange in part medial TM And Which other in part lateral. After position Which satisfying achieved, sponge gel foam is arranged around the graft border. 13,14
4 Complications Tympanoplasty
Studies have shown that tympanoplasty is successful in over 93% of patients (in patients undergoing primary tympanoplasty using a temporalis fascia graft). However, as with any surgery, complications can occur. The major complications of tympanoplasty include recurrence (this includes graft failure), conductive hearing loss, TM perforation, and intraoperative or postoperative ventilation tube placement.
A large case series analyzing more than 1000 patients undergoing tympanoplasty bone vulnerable, report relapse perforation TM on 3.6% until 4.2% of patients (patients with high-risk cholesteatoma and perforation) and conductive hearing loss requiring revision in 9% (high-risk perforation with/without cholesteatoma patients) to 11% of patients (patients undergoing TM repair for hearing improvement). In addition to the approach and graft choice, major contributing factors that may affect postoperative outcomes include patient comorbidities such as diabetes, smoking, and immunosuppression. 9
There is important nerve structures that cross ear middle, namely the facial nerve and chorda tympani. The facial nerve courses within the temporal bone and continues along the posterior wall of the tympanic cavity, above the oval window. Fortunately, iatrogenic injury to the facial nerve is very low due to the extensive training of otologic surgeons performing tympanoplasty. The chorda tympani will always be exposed during middle ear surgery, and in CSOM with cholesteatoma, the chorda tympani may have to be sacrificed to achieve complete clearance of the disease. 4,9
REFERENCE
Hassan S, Froschl U, Joseph S, Alamo A. Success Rate of Tympanoplasty in Chronic Suppurative Otitis Media Patients: A Retrospective Study at Saint Paul Hospital Millennium Medical College, Ethiopia. Austin J Otolaryngol [Internet]. 2021;8(1):1–
5. Available from: www.austinpublishinggroup.com
Hawkins JE. The Physiology of Hearing. In: Encyclopedia of Britannica [Internet]. Britannica; 2022. Available from: https:// www.britannica.com/science/ear/The- physiology of hearing
Brar S, Watters C, Winter R. Tympanoplasty. StatPearls [Internet]. 2023; Available from: https:// www.ncbi.nlm.nih.gov/books/NBK565863/%0A
Choi SW, Moon IJ, Choi JE, Bro WS, Moon IS, Kong SK, et a. Outcomes of
Endoscopic tympanoplasty for large perforations: A multicenter retrospective study in South Korea. Clin Exp Otorhinolaryngol. 2023;16(2):125–31.
Pap I, Kovacs M, The Bulges B, Szakács Z, Gerlinger I, Imreh B, et a. Quality-of-life outcomes with endoscopic and microscopic type I tympanoplasty—a prospective cohort study. Eur Arch Oto-Rhino-Laryngology [Internet]. 2023;280(10):4401–8. Available from: https://doi.org/10.1007/s00405-023-07938-6
Drawer D, Scroll I, Kuzucu I, Cum RO, Ozcan M. Type 1 tympanoplasty in pediatric patients: A review of 102 cases. BMC Pediatr. 2018;18(1):14–9.
Dispenza F, Battaglia AM, Salvago P, Martines F. Determinants of failure in the reconstruction of the tympanic membrane: A case-control study. Iran J Otorhinolaryngol. 2018;30(6):341–6.
Chen CK, Hsu HC, Wang M. Endoscopic tympanoplasty with post-conchal perichondrium in repairing large-sized eardrum perforations. Eur Arch Oto-Rhino- Laryngology [Internet]. 2022;279(12):5667–74. Available from: https://doi.org/10.1007/s00405-022-07476-7
Hassan S, Froschl U, Joseph S, Alamo A. Success Rate of Tympanoplasty in Chronic Suppurative Otitis Media Patients: A Retrospective Study at Saint Paul Hospital Millennium Medical College, Ethiopia. Austin J Otolaryngol [Internet]. 2021;8(1):15. Available from: www.austinpublishinggroup.com
Comments