LITERATUR REVIEW
I Made Nudi Arthana
Benign Paroxysmal Positional Vertigo (BPPV)
1. Anatomy And Physiology Organ Vestibular
Benign Paroxysmal Positional Vertigo (BPPV) is a disorder characterized by with vertigo repetitive Which caused by change position head such as looking up, changing position when lying down, or when trying to straighten the position body after bow, abnormality on ear in can causes vertigo. Labyrinth vestibular is part from ear in. Labyrinth This function for detect existence acceleration. Part from ear in that works to detect angular (rotational) movements is the KSS, while the one that functions to detect linear movements is the autolytic apparatus. 6
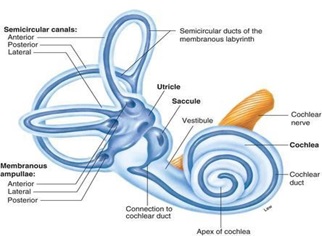
Picture 1. Bone And membrane labyrinth 3
Angular acceleration is detected by a structure consisting of three KSS, which occupy three spatial planes at certain angles. These three KSS are the anterior KSS, posterior KSS and horizontal KSS. Posterior KSS and anterior KSS approximately is at on position vertical. KSS posterior is at on position which is the same as the axis of the petrous bone (approximately 45 0 to the sagittal and coronal planes). The horizontal KSS is in a raised position of approximately 30 0 upwards. The tip of each KSS widens at its junction with the utricle. Part Which widen This called ampulla. In in ampulla there is a structure cell sensory Which consists of from Christ And cupula. Moment happen movement rotating, there is a stimulus that causes an arc-like movement in the cupula so that there is a shift in the sensory cilia in the cupula. The rotating movement stimulus in both the left and right ears is amplified in the vestibular nucleus mutually. opposite as reflection One The same other with mechanism each other push -pull . Nerve inhibition on one side of the ear (push) is always balanced by an increase in nerve impulses on the other side of the ear (pull) . 6

Picture 2. Ampula KSS 6
Linear acceleration is detected by a pair of otolithic apparatuses, namely the utricle macula and the saccule macula. These two maculae called organ static macula. In the upright head position, the utricular macula is approximately horizontal, while the saccular macula is approximately perpendicular to the utricular macula. Within the static macular organ are ciliary hair cells embedded in a gelatinous otolithic membrane. On the surface of this membrane are otoliths (also called otoconia or statoliths ), which are calcium carbonate crystals measuring 0.1-30 µm. Both of these otolithic organs function to detect linear movement that is not perpendicular to the macula. If linear movement occurs, it will cause the otolithic membrane to shift relative to the cells. sensory. Because both maculae are at an angle to each other each other, one of the two always gets stimulation from the force of gravity. Through this mechanism the otolithic apparatus detects the relative position of the head in space.
Benign Paroxysmal Positional Vertigo (BPPV)
2 Definition
Benign Paroxysmal Positional Vertigo (BPPV) is defined as a disease of the inner ear with recurrent episodes. BPPV is also often known as with abnormality on part vestibular. BPPV is disturbance clinical that often happen on individuals attack vertigo type peripheral, followed symptoms of dizziness, nauseous, vomiting and sweat cold that matter due to by reposition head oppose gravity without lesi on system center (Perdossi, 2017).
Vertigo is the perception of body movement and the environment caused by various conditions and vertigo, not just a symptom of dizziness, but a series of symptoms or syndromes that occur from somatic symptoms (nystagmus, untoble) autonomic (pale, cold sweat, nausea and vomiting dizziness more describes feelings or movements that are generally uncomfortable, shaky, to light and reactions that are difficult to describe by the sufferer themselves. Patients sometimes feel these symptoms and describe them as tingling, short-term dizziness (Sutarni, 2018).
3. Epidemiology
BPPV is the most common disorder of the peripheral vestibular system. According to research by Mizukoshi et al., 3 incidence figures for BPPV in the country Japan 10.7-17.3 per 100,000 person per year. On literature other It is stated that the incidence of BPPV is 10.7-64% per 100,000 patients per year. 4 Several studies also state that the incidence of BPPV is higher in women than in men, but other literature states that the incidence is the same between men and women. 3.5 BPPV often occurs at the age of 50-70 years, the risk increases in old age. BPPV most often affects posterior SCC compared to horizontal and anterior SCC. 2-4
4. Etiology
Part big case BPPV (50-70%) found as a case in point alone and termed as BPPV primary or idiopathic. BPPV secondary most often caused by Head trauma is 7-17% of all cases of BPPV. In Head trauma, shaking of the head causes the release of a number of otoconia into the endolymph so that often found complaint BPPV bilateral. On 15% BPPV cases are caused by viral neurolabyrinthitis or also called vestibular neuronitis. 3
Disease Meniere Also often associated with BPPV. Various literature has difference in terms of how big is the proportion patient BPPV who are also diagnosed with Meniere's disease. The range is approximately 0.5-31%. Gross et al. found that 5.5% of Meniere's patients were confirmed to have BPPV KSS posterior. Mechanism the cause is not yet known, but is thought to be the result of damage triggered by hydropic causes in the utricular macula or due to partial obstruction in the membranous labyrinth. 1-3
In recent cases, it has also been found that migraine is closely related to BPPV. Research by Ishiyama and Lempert found an increased incidence of migraine in BPPV patients and an increased number of recurrences. BPPV after success done positioning on patient migraine. Suspected mechanism the cause is spasm on artery in ear in, because vasospasm is clearly observed in migraine cases. 3
BPPV secondary often Also complained about by patient Which has undergo surgery ear in. The cause relate with damage utricle during surgery, which causes detachment of the otoconia. 3
5. Pathophysiology
BPPV is caused by the release of otoliths consisting of calcium carbonate from the utricular macula that detaches and moves within the lumen of one of the SCCs. Calcium carbonate is twice as dense as endolymph, so it moves in response to gravity and other accelerative movements. When these otolith crystals move within the SCC, they cause movement stimulating endolymph the affected ampulla of the KSS causing vertigo. 3,6 When the patient is in a position that causes vertigo, eye movements will appear caused by muscle contractions related to the affected KSS (slow phase) followed by a rapid corrective movement in the opposite direction (fast phase). This biphasic (two-phase) movement is called nystagmus. 2 The direction of nystagmus is influenced by excitation nerves in ampulla through connection direct to extraocular muscles. For each KSS that experiences this disorder will cause the emergence of a typical nystagmus (table 1). The free movement of calcium carbonate crystals in the KSS is called canalithiasis. While cupulolithiasis is a condition Which more seldom happen that is particle- calcium particles stick on cupula. There is a draft Which termed as “clock channels” where calcium particles sometimes move or sometimes get stuck in the canals. 3,6,7
Table 1. Characteristics nystagmus in accordance with KSS Which involved 7
KSS Which involved | Direction from nystagmus paroxysmal positional phase fast |
KSS Rear | Upward + torsional punching motion ( upbeating- torsional nystagmus) |
KSS Horizontal | Geotropic horizontal + Apogeotropic horizontal |
KSS Front | Movement downbeating + mild torsional nystagmus |

Picture 3. Canalithiasis And cupulolithiasis 3
The cause of the release of calcium crystals from the macula is not known for certain. Debris calcium can let go consequence existence trauma or infection virus, but often occurs without any trauma or identifiable disease. This may be related to the effects of age that cause changes in the protein and gelatin matrix of the otolith membrane . It has also been found that BPPV patients suffer more from osteopenia and osteoporosis compared to the control group, and in patients with BPPV tend to repeat have bone density which is very low. This is show that the release otolith (otoconia) spontaneously occurs together with general bone demineralization. 7
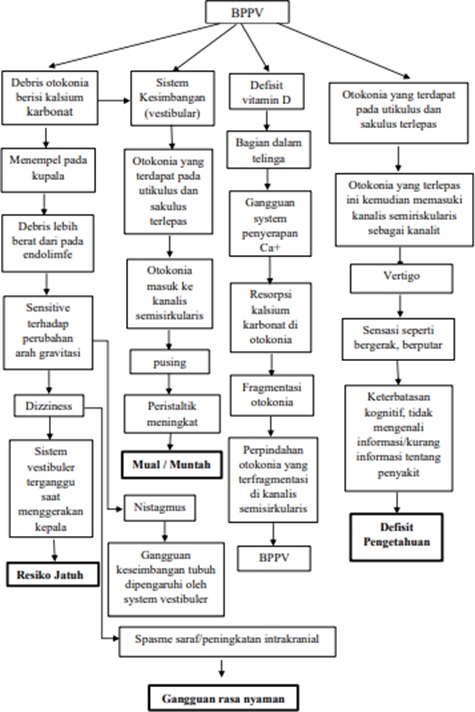
Picture 4. Pathway BPPV
6. Diagnosis
In general, the diagnosis of BPPV is established based on anamnesis and physical examination with diagnostic maneuvers. Through diagnostic maneuvers can provoke emergence nystagmus, so that can observed type, direction, And The duration of nystagmus can provide clues to the affected KSS and its mechanism. Inspection Which use chair turn And posturography not very useful in BPPV patients. Examination using CT-scan or MRI is not necessary unless there are unusual symptoms that require further examination. 2,3,7
Anamnesis
In the anamnesis, the patient felt sudden vertigo due to head movement/position. certain Which most often found during movement to rotate in place sleep, look up, And bow down. Patient can know vertigo Which due to by problems in the right/left ear with pay attention to the appearance of vertigo when rotating movements to the right/left, for example The patient feels dizzy when turning to the right bed, but not felt when turning to the left. Matter This show that vertigo is caused by by problem in ear Right. Vertigo attacks usually last less than 30 seconds, but some patients feel the duration of vertigo they experience lasts up to several minutes, but actually less than 30 seconds. This difference in perception may be caused by the fear experienced by patients accompanied by nausea and loss of balance when the attack occurs. 2,3,7,8
Patient Also Lots who complained of mild headaches, nausea, loss of balance, and feel sensitive to all movement head. Although 50-70% of BPPV cases are idiopathic, anamnesis is necessary to estimate the cause. secondary from BPPV, for example head trauma, viral labyrinthitis, or vestibular neuronitis, Meniere's disease, migraine, and otological/non-otological surgery. 3
Inspection
Inspection physique done with do maneuver diagnostic. There are two diagnostic maneuvers for BPPV, namely the Dix-Hallpike maneuver and the supine head turn maneuver (Pagnini–McClure maneuver). 2,3,6,8,9
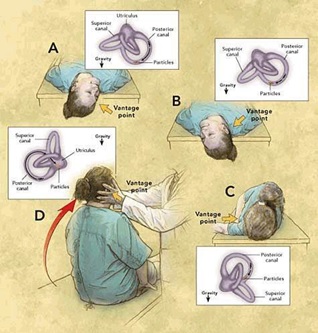
Maneuver Dix-Hallpike/Test Side- lying
It is a diagnostic maneuver for BPPV, both posterior and anterior KSS. aim For provoke attack vertigo and see the presence of nystagmus. The stages of this maneuver are as shown in figure 4.3
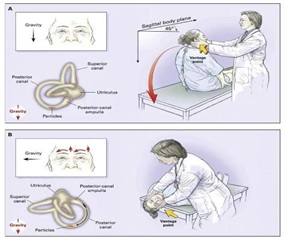
Picture 6. Maneuver Dix Hallpike (on ear right) 3
Picture 5. Test Dix- Hallpike 18
Test Side Lying Test This is test alternative Which easy used, can be adapted for patients with limited range of motion or who have difficulty relaxing. 18
Picture 6. Test Side -Lying
First, the patient sits in position A, then lies down in position B, and the patient's eyes are observed to see if there is nystagmus. After the head is lowered to position B, the onset of nystagmus usually has a latent period. the short one (1-5 second) and duration limited (usually less than 30 seconds). With the initial position of the eyes in the middle (neutral) position, nystagmus in posterior KSS BPPV has a vertical direction during the fast phase and also nystagmus direction torsional the strong one is in the fast phase of the top corner eyes hit to direction ear Which problematic. Mixture movement vertical And torsional This often referred to as upbeating-torsional nystagmus . Direction from nystagmus will reverse when the patient is straightened back to position A and then the nystagmus will experience fatigue. Along with the occurrence of nystagmus, the patient will feel vertigo with an intensity that matches the nystagmus response. It must be ensured second KSS posterior checked in a way separated, that is KSS posterior right checked with to move head to right And on the contrary KSS posterior left is checked by moving the head to the left. 2,3
BPPV KSS front very seldom occurs and its pathophysiology until At the moment not yet known. Its distinctive features is when the Dix-Hallpike test appears torsional downbeating nystagmus . The direction of the torsional nystagmus component indicates the affected ear. Patients with this type of nystagmus should be evaluated for the possibility of a central lesion, which is a rare case. 2,3
Supine head turn maneuver (maneuver Pagnini–McClure)

Picture 7. Maneuver supine head turn (maneuver Pagnini–McClure) to determine the presence of horizontal (lateral) BPPV KSS 7
Inspection For BPPV KSS horizontal done with supine head turn maneuver or also called the Pagnini–McClure maneuver, which is done by laying the patient in a supine position and then turning in a way fast head laterally towards the side being examined. Pure nystagmus horizontal will occur and be geotrophic (rapid movement towards the sea) ear which is below). Horizontal nystagmus can also occur apogeotrophically (directed to the ear above) but this is less common. 3
Compared to with Posterior BPPV has vertical-torsional nystagmus, in cases of horizontal KSS BPPV, the horizontal nystagmus has a latent period. more short with intensity Which more strong during inspection done. Both side must checked And direction nystagmus Which felt own The strongest intensity will indicate the problematic side and the causal mechanism (table 2). 3
Table 2.
Side problematic ears in horizontal KSS BPPV and the mechanism is based on the direction and intensity of the nystagmus. 3
Intensity nystagmus | Side ear Which problematic And mechanism BPPV | |
Nystagmusapogeotrophic | Nystagmusgeotrophic | |
More strong to side left | Cupulolithiasis right | Canalithiasis left |
More strong to side right | Cupulolithiasis left | Canalithiasis right |
In canalithiasis, head movement towards the affected ear causes particles to move towards the ampulla, triggering the onset of nystagmus where the fast component is towards the side of the ear being examined (the ear on the right). down). When the head is turned to direction side healthy ears, particles will move towards the opposite direction to the ampulla which can also trigger the emergence of geotrophic nystagmus but the intensity is lighter when compared to the ear on the affected side. 2 In cupulolithiasis, particles stick to the affected KSS cupula, so that these particles become more heavy from the endolymph, so that when head turned to one side so style gravity on Christ ampullary to move debris to direction the opposite side and nystagmus can be observed in the opposite direction from the ear being examined (apogeotrophic). 2,3,7,8
7. Diference Diagnosis
There are few other medical conditions that have symptoms similar to BPPV. In Meniere's disease, vertigo attacks are not triggered by changes in position and last longer (30 minutes to several hours). They are usually accompanied by tinnitus and hearing loss. Vertigo in labyrinthitis or Neuronitis vestibular usually in progress during a number of day and vertigo appears due to head movement in all directions, so it needs to be paid careful attention special on moment anamnesis. There is case Which very rarely, that is posterior fossa tumors have symptoms very similar to BPPV, but do not have similarity Which perfect with results positive inspection maneuver Dix- Hallpike . Need remember that BPPV can is condition secondary, so that it can appear in simultaneously or after the existence of disorders of the inner ear or central nervous system. BPPV often occurs coincidentally with other diseases. 3
8. Management
Management of BPPV with drug therapy, physical therapy, and in certain cases requires surgery. In general, the management of BPPV consists of from action without surgery And with surgery.Prognosis in general general is Good, Lots from condition BPPV own journey spontaneous profitable Because dysfunction peripheral vestibular tends to get better and because there is central vestibular compensation.
Action without surgery that is maneuver Liberator (maneuver Semont), particle repositioning maneuver, and horizontal BPPV KSS repositioning technique. Actions with surgery only done on cases Which very requires because BPPV is basically a harmless condition. Before surgery, imaging of the posterior fossa should be performed to see if there are central lesions that can cause symptoms similar to BPPV. Surgical procedures for treating BPPV include singular neurectomy and posterior SCC occlusion. 1-4,7-10
Drug Therapy
Medical therapy Vestibular-suppressant medications, such as antihistamines (Meclizine, dimenhydrinate), anticholinergics (scopolamine), or benzodiazepines (diazepam), may be given for short-term use in very symptomatic patients. These medications provide only symptomatic relief.
Without Surgery
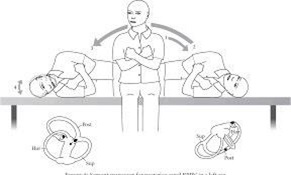
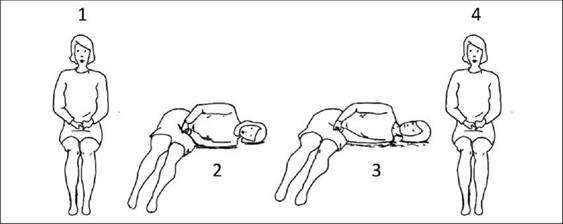
Maneuver Liberator (Maneuver Semont)
Picture 8. Maneuver Liberator (Maneuver Semont) 3
On year 1988 Semont and friends explain maneuver Liberatory (picture 6) based on theory cupulolithiasis. It is believed that a series movement for change position on head causes the release sticky deposit in the cupula. This maneuver begins by placing the patient in a sitting position and turning the head away from the affected side. The patient is then immediately placed in position lie down sideways to direction Which problematic, with position head facing to on. After around 5 minute patient quick lie down in the opposite direction through the sitting position path until the patient is lying on his side with face down. The patient is then held in this position for 5-10 minutes and then slowly returns to a sitting position. 3,7,10
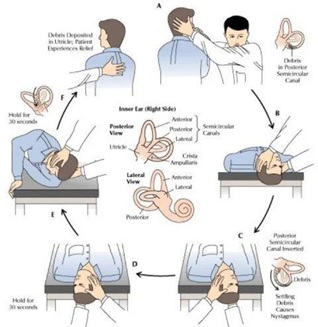
Maneuver reposition particle
On year 1992, Epley publish Canalith Repositioning Procedure (CRP) even though Epley had taught his technique for many years before. The Epley maneuver was performed with the patient Which sedation. Repeated vibrations were applied to the skull and the patient's head was moved through five different positions in sequence. 3Maneuver Epley can done with method as follows:
Done identification the side that problematic And done observation of latency and duration of nystagmus response.
Premedication use stock transdermal with diazepam or scopolamine.
A maneuver was performed to reposition the canalith in the right ear (for the left side do the opposite) as follows (figure 7):
The patient is in a sitting position, then directed to the right Dix-Hallpike position, causing the debris to move away from the posterior KSS cupula.
On moment patient is at in position supine, head patient played look to the left.
By maintaining the relative position of the head in relation to the left shoulder unchanged, body patient overthrown to direction left with rely on on shoulders and hips so that the patient's face faces the floor.
The head is maintained in a position turned to the left, with the head down and then the patient is woken up into a sitting position.
Then face patient rotated towards to front with chin looks down. Important to note that patient maintained in each position in on until nystagmus stop.change position head is performed when the nystagmus response stops. If there is no nystagmus, used estimation from amount latency And duration on previous response (usually 6-13 seconds) to determine When head position changes are made to next position. Nystagmus should be observed in all positions because if there is a change in the direction of nystagmus it indicates a failure of the placement of debris deposits in the vestibule.
Oscillation was performed using an oscillator with a frequency of 80 Hz which was applied to the mastoid process on the affected side.
Patient recommended For maintain position upright during 48 O'clock. This procedure can be repeated in weekly intervals until there are no more symptoms and no nystagmus is observed. According to Epley this procedure causes otolithic debris to move by gravity from the posterior SCC to the utricle. 3,7,9
Picture 9 . Maneuver Epley ( Canalith Repositioning Procedure ) 4
Picture 10. Maneuver reposition particle 3
Part big doctor moment This use technique CRP Which modified. One of the modified CRP techniques is the particle repositioning maneuver. namely maneuvering through three positions so that sedation and mastoid vibration are no longer required. With a good understanding of inner ear anatomy and pathophysiology from BPPV, power health including doctor family And Physiotherapy will be able to perform these particle repositioning maneuvers well.
Procedure maneuver reposition particle done with method as following:
Patient placed in position Sit down.
Patient moved to position head hang Dix- Hallpike to direction problematic ears.
Observe existence nystagmus stage beginning on eye patient.
Patient left alone on position This during 1-2 minute (position B).
Head patient played 90º to direction position Dix Hallpike Which opposite while maintaining the neck position in full extension (position C).
Then round added 90º until head patient reach position D diagonally opposite the first Dix-Hallpike position. The change from position B through C to position D should take no more than 3-5 seconds.
Immediately observe the patient's eyes for secondary nystagmus. If the particles continue to move one way ampulofugal, through the intersection that The same going to to in utricle so nystagmus secondary This should be in line with nystagmus primary.
The patient is kept in the above position for 30-60 seconds and then the patient is instructed to sit down. If the maneuver is successful, there should be no nystagmus and no vertigo when the patient is in the sitting position because all the particles have returned to the utricle. 3
In general overall maneuver This in progress during 5 minute until completed. The patient is then usually asked to remain upright for 24-48 hours to allow the otolith to adhere properly so that there is no recurrence. 3
Technique reposition BPPV KSS Horizontal
There are several repositioning techniques for horizontal SCC BPPV. The simplest is the technique developed by Vannucchi et al. called prolonged position maneuvers . Maneuver This done especially in observed cases the presence of geotrophic nystagmus where the patient is laid on his side with the affected ear facing up for 12 hours. There is also the “Barrel roll” technique described by Epley, namely by rotating the patient 360º from position supine back to supine position, keeping the KSS position horizontal perpendicular to the floor. Rotation is done in the opposite direction to the position of the problematic ear. Rotation is done gradually as far as 90º until one full rotation is completed. This method causes the particles to move out of the problematic canal towards the utricle. 3

Picture 11 . Maneuver Lempert (Maneuver Log Roll ) 7
For patients who have more difficulty moving, Lempert and Tiel Wick designed a maneuver called the “Log Roll” . In this technique the patient’s head is turned completely toward problematic ear. Then the patient rotated rapidly in the opposite direction with the problematic ear gradually 90º to total round 270º. For each stage of position 90º, the head patient let stand for 1 minute. 3.7
Vannucchi's Forced Prolonged Position
This maneuver is used in horizontal canal type BPPV with severe symptoms. getting worse with change position And No clear where ear affected.

Picture 12. Vannucchi's Forced Prolonged Position
Guffoni Maneuver
Maneuver guffoni done on BPPV involving channel horizontal with apogeotropic nystagmus
Picture 13. Guffoni Maneuver
Jacobino Maneuver
This maneuver done on patient with duration nystagmus ≥ 1 minutes, the holding time of each body position is extended appropriately. The maneuver is repeated if symptoms do not improve or if reduction fails.
Picture 14. Jacobino Maneuver
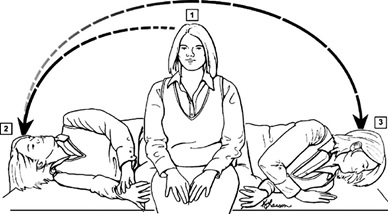
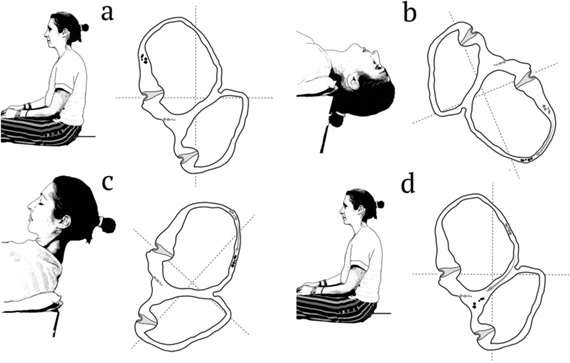
Exercise Brandt -Daroff
Exercise daroff brand can smooth the flow blood to the brain so as to be able to repair system vision, system balance ear in And system sensory Good movement, pressure And position (Fauziah, 2015).
Brand daroff can generally be applied when vertigo is not clear. Brand baroff has the effect of increasing blood flow to the brain, increasing the role of the body's balance tools and increasing the activity of the sensory system. Brandt daroff has the advantage of eliminating stimulus reactions in the form of unpleasant sensations and moving perceptions in the brain, and helping to reposition in crystals located in the semicircular canals. Brandt Daroff exercises for physiological adjustments use to enhance the influence of adjustment and habituation of the vestibular system, and Brandt Daroff exercises have an effect on the adjustment process at the degree of sensory integration. Sensory integration Also functioning on adapt repeat input Which No balanced, vestibular organ And perception sensory other. Move otokonia For Return to the utriculus through the non-ampulatory end of the canal with the help of gravity. The output from the physiological adaptation mode activity is to improve balance and reduce the risk of falling (Hastuti Puji Tri, 2017).
Brandt Daroff is a therapy that can be done by yourself in the following ways (Srinivasan, 2020):
First do with Sit down upright side place Sleep
Lie down adjacent right. With time less than 1 or 2 seconds
Look head 45 degrees in One direction (eg left)
Do during 30 second or until vertigo subside e. Position upright or sit and wait 30 seconds
Then lie on the other side towards the left do less than 1 or 2 seconds with a 45 degree head turn in one direction
Still in position the, 30 second or until vertigo subside
Return on position sit down and Wait during 30 seconds or until subside.
Each treatment takes 10 minutes, one set consists of 5 repetitions.

Picture 15 . Exercise Brandt- Daroff 2
The Brandt-Daroff exercise is done with repeated movements, namely from a sitting position then lying on your side towards the affected ear, then... silent on position the wait until vertigo is lost, Then back to position sit down. This movement can be repeated in the opposite direction if it is not known which ear is problematic. 9
Classic manual repositioning is an effective and recommended treatment. by guidelines American Academy of Otolaryngology-Head and Neck Surgery , for posterior semicircular canal BPPV (Epley maneuver), horizontal canal BPPV half circle (maneuver barbecue), And Cupulolithiasis BPPV horizontal canal (Gufoni maneuver). 18
Table 3 . Diagnosis And order like BPPV seen from KSS affected by 18
KSS Affected | Maneuver | Type Nygtamus | Management Options |
KSS Rear | Dix Hallpike | Torsional Upbeating nystagmus | ManeuverEpley |
KSS Horizontal a. Geotropic |
Supine Head |
Beatingto direction ear |
|
b. Apgeotropic | Roll
Supine Head Roll Dix Hallpike | most lower
Beating to direction bottom ear Paroxysmal Downbeating nystagmus | Barbecue
ManeuverGufoni
Jacobino Maneuver |
Surgery
Neurotomy Singular
Singular neurectomy (cutting of the posterior ampullary nerve) serves to send impulses from the posterior KSS to the part of the brain that functions in the system. balance. Technique This developed And introduced by Gacek in the 1970s. Initially Gacek reported high efficacy but reported there is a significant risk the occurrence neurosensory deafness (SNHL). This procedure is considered requires technical skills very high that cause this technique replaced by technique Which more simple, namely the posterior KSS occlusion technique. 3
Occlusion KSS Rear
Technique This based on by draft that clog cavity on channel KSS will inhibit the flow of endolymph which effectively repairs the cupula into no longer responsive to pressure acceleration normal angular. Which is more the important thing is to be No responsive to stimulation from particles Which move free in in endolymph and also particles attached to the cupula deposit. Initially this procedure was considered too dangerous Because done to ear with hearing Which normal, but studies by Parnes and McClure demonstrated that This procedure does not cause any effect on hearing. Procedure This done with anesthesia general in time which is no more than 2-3 hours. Perform a 5-6 cm post-auricular incision for access KSS posterior through mastoidectomy. With using a microscope And drill fenestrated size 1 mm x 3 mm on bone posterior canal, then a plug is made to occlude the canal. The plug is made with a mixture of bone dust using fibrinogen adhesive. Most patients will be hospitalized for 2-3 days after the procedure. On at first patient will experience disturbance balance post-operatively. The patient's brain will adapt after a few days to a few weeks and can be helped by doing vestibular physiotherapy. 3

Picture 16. Algorithm order like BPPV with Maneuver reposition channel 18
7. Prognosis
Success therapy depends from accuracy identification from KSS affected, can differentiate between canalithiasis and cupulolithiasis and the choice of appropriate maneuver. The effectiveness of Liberatory maneuver and particle repositioning is 70-100%. Recurrence of symptoms after remission is complete varies between 4-32%. 2 The examiner must be careful when performing diagnostic maneuvers, maneuver Liberator and also reposition particle on patient obesity with limitations motion on area cervical or on patient with heart failure or carotid stenosis. 2
Some researchers believe that patients with pure BPPV can recover spontaneously, with more than 89% of patients recovering spontaneously within the first month. And 33% experience relapse after 3 years. Resolution Spontaneous can occur more quickly in horizontal KSS BPPV compared to BPPV KSS posterior Because formation room Which facilitate particle to its place of origin. So that the patient can be advised to wait for spontaneous healing, especially in cases where therapeutic maneuvers cannot be performed. 2
CONCLUSION
BPPV is a condition where there is a disturbance in the peripheral vestibular system, when patient feel sensation Dizzy turn And move which is associated with nystagmus when the position of the head changes with respect to the force of gravity. And accompanied by symptoms of nausea, vomiting, And a cold sweat. BPPV is characterized by sudden, brief episodes of vertigo triggered by certain head movements that usually occur due to the displacement of calcium-carbonate crystals or otoconia. in in semicircular canals contain fluid in inner ear. The diagnosis of BPPV can be established based on anamnesis and physical examination through diagnostic maneuvers. Management of BPPV generally consists of non-surgical and surgical measures. The management that frequently used are non-pharmacological which include several maneuvers such as Epley, Semount maneuver and Lempert maneuver.
REFERENCE
Brandt T, Arnold W. Benign Paroxysmal Positional Vertigo in: Arnold W editor. Vestibular Dysfunction and Its Therapy. Munich-Germany: S.Karger.AC;2019.p.169-194.
Bittar RSM, Mezzalira R, Furtado PL, Venosa AR. Benign paroxysmal positional vertigo: diagnosis and treatment. International Tinnitus Journal.2017;16(2):135-45.
Parnes LS, Agrawal SK, Atlas J. Diagnosis and management of benign paroxysmal positional vertigo. JMAC.2013;169(7):681-93.
Kim JS, Zee DS. Benign paroxysmal positional vertigo. The New English Journal of Medicine. 2017;370:1138-47.
Ogun OA, Janky KL, Cohn ICE, Lunberg YW. Gender Based Comorbidities in Benign Paroxysmal Positional Vertigo. Plos One. 2018;9:1-8.
Probst R, Grevers G, Iro H. Vestibular Disorders in: Basic Otorhinolaryngology. 2nd ed. Stuttgart-New York: George The World Translation; 2016.p.272-86.
Fife TD. Benign paroxysmal positional vertigo. Seminars in neurology. 2019;29(5):500-08.
Brandt T, Dieterich M, Struggles M. Benign Paroxysmal Positioning Vertigo in: Vertigo and Dizziness. United States of America: Springer-Verlag LondonLimited; 2017.p.41-61.
Desmond AL. Treatment of Vestibular Dysfunction in: vestibular Function: Evaluation and Treatment. Stuttgart-New York:Thieme 2018.p.111-147.
Libonati GA. Benign paroxysmal positional vertigo and positional vertigo variants. Otorhinolaryngology clinics: An International Journal.2019;4(1):25- 40.
Hornibrook J. Benign Paroxysmal Positional Vertigo (BPPV): History, Pathophysiology, Office Treatment and Future Directions. International Journal of Otolaryngology. 2021;11:1-13.
Kyoung DY, Kim J, Park CY, Chung MH. The Effect of Early Canalith Repositioning on Benign Paroxysmal Positional Vertigo on Recurrence. Clinical and Experimental Otorhinolaryngology.2019;4(3):113-17.
Yu S, Liu F, Cheng Z, Wang Q. Association between osteoporosis and benign paroxysmal positional vertigo: a systematic review. BMC Neurology. 2017;14(110):1-6.
Balatsouras DG, Koukoutsis G, Ganellis P, Corresponding author GS. Diagnosis of Single- or Multiple Channel Benign Paroxysmal Positional Vertigo according to the Type of Nystagmus. International Journal of Otolaryngology.2018;1-13.
Solomon D. Benign paroxysmal positional vertigo. Current Treatment Options in Neurology.2020; 2:417-27.
Moreno JL, Munoz RC, Balboa IV, Matos YR, Agudelo OL. Effectiveness of the Epley's maneuver performed in primary care to treat posterior canal benign paroxysmal positional vertigo: study protocol for a randomized controlled trial. Trials Journal.2017;15(179):1-10.
Winda G, Sinta M, Kusumaningsih D.2022. Management of Benign Paroxysmal Positional Vertigo (BPPV). Surakarta: Muhammadiyah University of Surakarta.
Bambang S, Muyassaroh. 2022. Benign management paroxysmal positional vertigo. Semarang: Dr. Kariadi General Hospital, Semarang.
Yue Lou, Miiao Cai, Liangguo Xu, Yanwen Wang, Liying Zhuang, Xiaoli Liu. 2020. Efficacy of BPPV diagnosis and treatment system for benign paroxysmal positional vertigo. American Journal of Otolaryngology. Volume 41, Issue 3
Hyo JK, JaeHan Park, Ji-Soo Kim. 2020. Update on Benign Paroxysmal Positional Vertigo. Journal of Neurology https://doi.org/10.1007/s00415- 020-10314-7
Yan E, Yelvita R. 2014. Diagnosis and Management of Benign Paroxysmal Positional Vertigo (BPPV) Horizontal Based on Head Roll Test. Andalas Health Journal.
Comments